

This infographic identifies ways to raise awareness among and better engage the LGBTQ+ community in clinical research and healthcare.
Additional Resources:
Read Broadening the Lens of Diversity for More Inclusion in Clinical Research | Written by Malia Lewin, Teckro
Read Improving LGBTQ+ Inclusivity in Ovarian Cancer Care | Written by Clara MacKay, World Ovarian Cancer Coalition
Read Considerations for LGBTQ+ Inclusion in Clinical Research | Industry Report written by Teckro

Written by: Kristen Castillo
The Havert family is taking on a major health diagnosis and taking care of each other along the way.
Aaron Havert, 40, and daughter Eleanii, 9, both have Hemophilia A, a genetic bleeding disorder caused by a lack of blood clotting factor VIII. The main symptoms of Hemophilia A include prolonged bleeding and bruising. Aaron’s case is considered severe while Eleanii’s case is considered mild. There’s no cure for Hemophilia A, but gene therapy may help reduce the severity of the disorder.
Aaron, who was diagnosed when he was 10 months old, needs to prevent a spontaneous bleed from occurring. He treats his Hemophilia A with factor infusions administered directly into a vein at home every two to three days. Eleanii receives factor treatment on demand, meaning she’s treated when she has a bleed.
Caregiving and advocacy
Melanie Havert, Eleanii’s mother, is a caregiver to both her daughter and to Aaron. The family lives in Northern California with their older daughter Charlii, age 11, and three pets.
Melanie, 36, started her caregiver journey in 2004 when she first met Aaron. He taught her at his kitchen table how to infuse him with life-saving intravenous injections.
“According to both Aaron and Eleanii, I am the best at giving infusions,” she says. “Without the factor being administered into their veins, Aaron would die, and Eleanii would have a very painful life and could even lose her life in the case of something like a minor head injury.”
Melanie’s caregiver role also includes giving Eleanii subcutaneous injections into her thighs; ordering medication and supplies; and attending appointments, conferences, and support groups. She’s often a resource for other new caregivers.
When she realized how little information was available about female Hemophiliacs like her daughter, she committed to connecting with female symptomatic carriers of the disorder.
Melanie is also a project manager at Rare Patient Voice, a market research recruitment firm providing patients and caregivers with opportunities to share their opinions and experiences with researchers.
Clinical trials
Aaron has participated in five clinical trials over the past 30 years, including four for different anti-hemophilic factors (AHF) and one for a first in-human gene therapy trial.
He participates to help improve treatment for Hemophilia. The condition can be difficult, causing physical limitations, chronic pain, and very expensive medical costs. His monthly medication costs $20,000.
A better future
When considering participating in clinical trials, Melanie advises patients and their families to understand the risks, ask questions, and speak with others who’ve participated to gain a better understanding of the process.
She also advises preparing the family for all possible outcomes and discussing it as a unit. A clinical trial has the potential to affect the entire family. When Aaron wants to participate in a clinical trial, he and Melanie have a long discussion of the possible risks. If he decides to participate, he writes a personal letter to each of their daughters explaining exactly why he decided to participate and what he hopes will come out of it.

CISCRP hosted a 3-part webinar series titled “Navigating Rare Disease and Clinical Research: Every Patient Matters”. This article brief is based on the second episode, “Rare Disease Clinical Trials: How to Prepare for When the Clinical Trial Ends”. Moderated by Joan Chambers, Senior Director, Marketing and Outreach, CISCRP and Marsha Lanes, Genetic Counselor/Medical Editor, NORD (National Organization for Rare Disorders), panelists included Dr. Tracy Dixon-Salazar, Executive Director, Lennox-Gastaut Syndrome (LGS) Foundation, Richie Kahn, Senior Director, Patient Engagement, Medable, Inc., and Dana Holinka, Operating Board Member, Tuberous Sclerosis Complex (TSC) Alliance. You can access the webinar recording here.
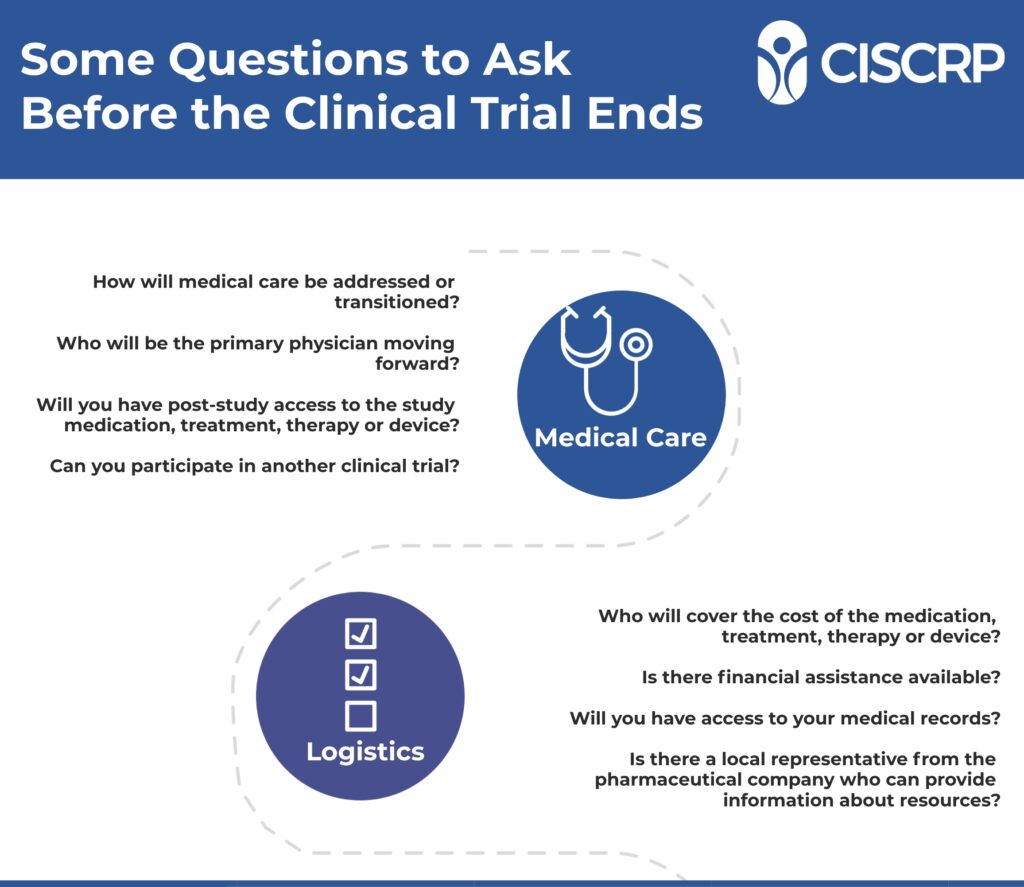
You or a loved one is participating in a clinical trial, which at some point, will come to completion. There are several considerations to address before the end of the clinical trial, and conversations to have with the PI (Principal Investigator) and clinical site staff. These include how medical care will be transitioned, who will be the primary physician moving forward, post-study access to medical records and study staff, access to study medication, how you will be informed about the outcome of the clinical trial and potential options to enroll in an upcoming clinical trial. In rare disease clinical research, participants are often minors, so caregivers and patient advocates may have additional questions.
“Don’t think that any question is silly, stupid or dumb, because you’re going to go into this transition phase feeling like you have no control, after you’ve been taken care of and guided along,” says Dana Holinka, whose daughter is a rare disease clinical trial participant.
Dr. Tracy Dixon-Salazar’s daughter has participated in 26 rare disease clinical trials for medications, treatments, alternative therapies, and diet. Tracy advises to ask questions about access and care. If the participant received the study medication and not the placebo, and was benefitting from it, ask if they will still have access to it.
In a clinical trial, the participant is cared for by the physician investigator and research staff, in addition to the standard of care that is concurrently being provided by their primary care physician. Once the trial is completed, ask how care will be transitioned, and if there is an option available to remain in the care of the study staff.
“How are you going to work with our primary care provider to make sure there is no gap, if the medication is something we want to stay on?” says Tracy. Other considerations are whether the study medication will be covered by the participant’s medical insurance and the length of access to it.
“People who are conducting clinical trials are the best of the best,” says Tracy. “They’re going to know very much about the research, very much about the treatment you’re on, and they’re going to know a lot about the process. Our experience, in the multiple trials that we have done, was that we could stay, if our insurance (in the United States) was now going to cover the medication. We had to work that out.”
Richie says another key for a successful transition is to “Prepare yourself to advocate, either as a patient or a caregiver, for a friend or loved one participating, and do it early.” Conduct research on clinical trials and the informed consent process, to make sure that all your questions get answered at the onset of the study, and that you understand exactly what is involved.
“Sponsors aren’t necessarily bound to continue providing access (to a treatment) after a trial ends. But when you’re having that conversation during the informed consent process, within that informed consent form, itself, all of this should be outlined. It’s good to check. If you are not sure, you can always reach out to your site coordinator, your PI (Physician Investigator). Often times, there are open label follow ups, long term extensions, and a couple of other possibilities, as well, where sometimes an investigational product will be made available after the trial wraps up. That is especially common after early Phase and first-in-human trials,” says Richie.
Biopharmaceutical companies and drug sponsors may have programs to assist families with the extra cost of the medication, after the clinical trial ends. This is dependent upon whether the product is already approved and marketed. There are other tools available, including state-level medication assistance programs. For investigational products that are not yet approved, there are mechanisms where a pharmaceutical company may be able to intervene to continue providing the investigational product after the clinical study concludes. And there may be the possibility of participating in another clinical trial. If a participant has not yet received the investigational medicine during the clinical trial, there may be an open access arm available at the end of the trial.
“Sponsors really do try to make that happen, as much as possible,” says Tracy.
Dana emphasizes the importance of networking with other patients, patient advocates, caregivers and advocacy organizations.
“Parents, and having those connections in the community, have helped us immensely. Connecting with other families and other people who are experiencing what you’re experiencing is huge. You can get some of the best information,” says Dana. This can include medical articles about the latest developments, or resources to help navigate day to day details. For example, Dana learned about a financial assistance resource called needhelppayingbills.com from another rare disease parent.
Dana recommends connecting with a local representative from the pharmaceutical company that can help with questions or concerns if there is one in your area.
“I think it’s imperative that you make those kinds of connections,” says Dana. “You can make them at the beginning, when you’re in the trial, or with some of the questions towards the end. Find out who that person is locally. They’ve had the experience of interacting with other parents, caregivers and the people involved in the studies.” The representative may be able to offer resources, such as discount coupons for medications or assistance with grassroots fundraising efforts.
“Generally, this is a really collegial industry. I think for just about everyone, it’s all about making those connections for the good of the patient. If you can get to the right person, you’re going to have a warm reception,” says Richie.
How information is shared with clinical research participants at the conclusion of the study is outlined during the informed consent process. If there are multiple sites and institutions involved in the clinical trial, enrollment rates and timetables may impact when the results of the clinical study are shared. The information has to be collected and analyzed. You can find information on clinicaltrials.gov and from advocacy groups and non-profits in your respective indications and therapeutic areas.
“Many sponsors will share this information directly with patients, if you ask,” says Richie.
“I think no matter where you live, if you are a patient in the trial or a caregiver, we all tend to have the same exact questions,” says Tracy. “Thinking about transitioning is a really anxious time for patients and families. Having those conversations start early, about the questions we’re all going to have, is really important.”
To learn more, you can view the webinar here. Access the companion infographic here.
You can view part-one of the series, “Rare Disease Clinical Trials: Being Informed About Clinical Research” here and part-three, “Rare Disease Clinical Trials: After Participation, Paying It Forward” here.
Access the companion infographics:
Authored by: Melissa E. Daley, Communications & Marketing Manager, CISCRP
To search for medical conditions in a specific location, visit our Search Clinical Trials page.
To stay informed about clinical trials, visit our Resources page.

The Clinical Trials Supplement features a variety of informative and timely articles about clinical research. This supplement covers clinical trial participants’ selfless gift to medicine, how African-American men can beat the adds against prostate cancer, exciting developments on an Alzheimer’s cure, and Otsuka’s holistic approach on clinical research.
The medical hero spotlight cover story features Mel and Aaron Havert, a patient and caregiver that are taking on a Hemophilia A diagnosis.







To participate in this campaign or an upcoming media campaign, please contact Matt Steele | msteele@ciscrp.org.


Authored by: Melissa Daley | mdaley@ciscrp.org
Richie Kahn shares, “I am a public health professional by training, and a clinical researcher by trade. I was working in full-service ophthalmology, developing new products for the eye, when I found out I was losing my vision.” It was March of 2019. Initially, it appeared that Richie had an early onset, clear-cut case of glaucoma, but a very different diagnosis lay ahead.
The diagnosis of glaucoma was initially confirmed through exams with an optometrist and an ophthalmologist who specializes in the disease. The ophthalmologist said that the good news was that they knew what Richie had, and the better news was that there were excellent treatment options available.
Richie shares insights on how technology can remove barriers to participating in clinical research.
Richie’s keen sense of humor shines through with his response to the ophthalmologist. “Well, I said bad news and worse news. Bad news, my background is in patient advocacy, and worse news is that I work in ophthalmology and know just enough to be dangerous, so I am going to be a giant pain in your butt,” smiles Richie. “Based on the fact that my doctor laughed, I knew we were going to get along well.”
Richie explains that “Glaucoma is a disease of the eye characterized by a build-up of fluid which causes increased pressure on the optic nerves connecting the eye to the brain. I decided this was an opportunity to turn lemons into lemonade, to build awareness of clinical research as a care option, and to get people screened for symptom-free vision loss.”
He used his skills and experience in business development in clinical research to conduct outreach to non-profits, particularly the Glaucoma Research Foundation, to ask how he could help. “If I have the opportunity to combine my knowledge of research and my passion for patient advocacy, put me in coach, I’m ready,” Richie says.
At an industry conference in the autumn of 2019, Richie met a key opinion leader (KOL) in the glaucoma field, who invited Richie to meet with him to review his case. This was the third medical opinion Richie had sought. Richie’s care team had performed the necessary screenings and followed treatment guidelines for glaucoma.
In that appointment, Richie received disturbing news.
“With relatively few signs and symptoms, I had lost about 15% of my vision,” says Richie. “That was the first indicator that what I had was not, maybe, so clear-cut.”
Richie’s optic nerve was pale, and the doctor was concerned. Tests were conducted to determine whether Richie had suffered a series of small strokes or had a tumor. Just after Thanksgiving in 2019, the test results came back negative. The KOL recommended that Richie confer with a neuro-ophthalmologist that was in the same building. After a lengthy appointment that didn’t provide any further insight, the neuro-ophthalmologist recommended genetic testing.
“I could hear from the tone in this doctor’s voice, he was not familiar with the diagnosis he was sharing,” says Richie. The doctor told Richie that the genetic tests indicated that he had Wolfram Syndrome, and that he should meet with a genetic counselor. Richie asked for his test results and he started researching the disease on his own.
NORD (National Organization for Rare Disorders) describes Wolfram Syndrome, in part, as “…an inherited condition that is typically associated with childhood-onset insulin-dependent diabetes mellitus and progressive optic atrophy. The symptoms and rate of progression of Wolfram Syndrome can be quite variable. Neurological symptoms such as poor smell, poor balance, an awkward, unbalanced way of walking (ataxia) and central sleep apnea can occur.” It also impacts the brain stem and affiliated critical bodily functions, including breathing. (Source: https://rarediseases.org/rare-diseases/wolfram-syndrome/)
“I used to go to a Korean Buddhist temple, for 15 years. So I am very much ‘It is what it is.’ You know, having good vision is temporary. Being alive is temporary. I was very matter of fact about it,” says Richie.
Richie decided to contact the KOL on Wolfram Syndrome, Dr. Fumihiko Urano, MD, PhD, of the Washington University School of Medicine in St. Louis, Missouri, and received a response. A meeting was scheduled with Richie, his wife, Dr. Urano and the clinical research nurse. Dr. Urano determined that Richie did not have Wolfram Syndrome but had Wolfram-like Syndrome.
“And I said, what is that?” says Richie.
Wolfram-like Syndrome is a rare disease, a disorder of the endoplasmic stress reticulum. It typically manifests between the ages of 6 and 8 years old, with optic atrophy that is often slow progressing. Later, many individuals develop insulin dependent diabetes. Sensory and other hearing loss may also occur.
“My particular flavor of the disorder, I was told by Dr. Urano, was only discovered by science in 2019,” says Richie. “I am patient number 17.”
The other 16 individuals presented symptom onset more typical of Wolfram-like Syndrome.
“Here I am, a unique and special snowflake, just like everybody else with a rare disease, right?” smiles Richie. “We have no way of knowing what the progression will be like. Eight or nine months after chatting with Fumi (Dr. Urano) for the first time, I had lost 15% of my vision. Today, I have lost almost 50%. So we’re preparing for legal blindness, I mean, I could be there right now. It depends on the test you take. But again, I am using this as an opportunity to focus on incorporating the patient perspective into clinical trial designs, creating studies that are less burdensome and building awareness of the whole thing.”
Wolfram-like Syndrome is an orphan disease, without any treatment and currently no clinical trials being conducted. Richie has connected with Amylyx Pharmaceuticals, in Cambridge, Massachusetts, a company that has been granted Orphan Drug Designation for AMX0035 for the treatment of Wolfram Syndrome.
“I’ve connected with the key opinion leader and looking to connect with patients — anything I can do to help make their lives easier and bring promising new therapies to them. It’s a net win,” says Richie.
Richie further explains that research indicates that up to 3% of individuals of western European Jewish heritage (Ashkenazi) may be carriers for this genetic condition.
“It makes me scratch my head,” says Richie, “because some might manifest with diabetes and no vision loss. Some might think they have glaucoma but they’re not diabetic. So I wonder how many patients might conceivably have this condition and just are not aware.”
“For vision loss, while there’s really fantastic work being done, through the Catalyst for a Cure program at Glaucoma Research Foundation, and there’s a lot of really promising pre-clinical work right now, once you’ve lost your eyesight, in almost every scenario, it is what it is. It’s not reversible. So I’m not necessarily looking at this (upcoming) trial to restore vision loss, or anything like that, for me. If I can contribute and help the next patient, fantastic. If I can at least build awareness about clinical research as a care option, and research even being an option in the community, that’s great. But I am not counting on my disease progression slowing or vision restoration. It’s more about building awareness of research, for both patients and clinicians, contributing to science and work in vision restoration.”
Richie’s patient advocacy efforts include public speaking engagements and work with the Glaucoma Research Foundation. “I am very clear now, about my diagnosis, in presenting myself as an optic atrophy patient and not a glaucoma patient,” says Richie. He is involved in the foundation’s patient summit steering committee and often moderates webinars and panels with the team.
Richie has high praise for the Glaucoma Research Foundation, saying “They’ve been absolutely lovely. They’ve connected me with other patients who are interested in becoming advocates, interested in writing blogs and sharing their perspective with researchers, which is fantastic. I am not only working with tremendous advocates, I have the opportunity to connect with patients and hear their stories, help them become better advocates, learn from them and just be a sounding board for them. Sometimes they’re just looking to vent. Ultimately, if they’re interested, I try to get them to be engaged and empowered to be their own advocates.”
Richie has participated in other non-vision-related clinical trials in the past, including a traditional brick and mortar clinical trial for migraine headaches. He participated in a one-day trial for involving a virtual reality headset, powered by artificial intelligence, that runs at-home visual field exams. He also tried, unsuccessfully, to participate in the recent COVID-19 vaccine studies, but did not receive calls back, most likely due to clinical site bandwidth.
When he shared with family and friends that he may participate in an upcoming clinical trial for Wolfram-like Syndrome, he did face some confusion from his loved ones. “A question I have heard is, ‘If you’re not going to restore your eyesight, then why would you participate?’ I try to use it as opportunity to educate, that everyone’s rationale and motivation to participate is different,” Richie explains.
Richie advises individuals considering clinical research that “If you’ve got questions about a clinical trial, reach out to the study site to get your questions answered. If you’re really curious, go through the pre-screening process. Go through screening. If you qualify, go through informed consent. Learn as much as you can, to make sure that, if you are going to participate, your expectations are clear. There’s nothing worse than either a patient or a doctor getting involved in clinical research and not having a clear understanding of what the study involves. And then share your experiences with your friends, family and community members.”
In June of 2021, Richie participated as a panelist in the CISCRP webinar titled “Rare Disease Clinical Trials: How to Prepare for When the Clinical Trial Ends”, where he shared his experience as a rare disease patient, patient advocate and clinical research professional. You can access the recording here.
Richie is very hopeful about the evolving state of the clinical research enterprise. “If there is a silver lining in the pandemic as it relates to clinical research, I think we’re at this inflection point where the momentum is such that we are moving towards decentralized trials, hybrid trials, where patients can participate, not necessarily 100% on their own terms, but from where they are situated and when they are able to participate,” says Richie.
To search for medical conditions in a specific location, visit our Search Clinical Trials page.
To stay informed about clinical trials, visit our Resources page.

Relevant resources:
If you are interested in licensing this infographic or other CISCRP content, please contact at info@ciscrp.org.
Authored by Melissa E. Daley, Communications & Marketing Manager, CISCRP
Clinical trials are standard common practice in cancer treatment for children, adolescents and young adults (AYA). The RACE (Research to Accelerate Cures and Equity) for Children Act requires that medications that are used to treat adult cancers also be assessed for use in pediatric populations, if certain criteria are met. SMEs from ICON, a global provider of consulting, and outsourced development and commercialization services to pharmaceutical, biotechnology, medical device and government and public health organizations, and Children’s Minnesota shared their experiences treating adolescent and young adult populations in light of the RACE for Children Act in a 15-minute Flash Webinar.
“Pediatric cancer is quite a different clinical area. When a child to young adult is newly diagnosed or has relapsed or refractory cancer, providers first look to clinical trials for recommended treatment,” says Missy Hansen, MSN, APRN, CPNP, CPHON, Pediatric Strategy Liaison, Center for Pediatric Clinical Development, ICON a former nurse practitioner now working in pediatric clinical development. “Even if there isn’t an open trial for the child to be enrolled on, providers will often recommend treatment according to a trial, if that trial is what we know to be the best treatment option for that child’s disease.”
It’s important to provide clear and complete information about clinical research participation to parents, caregivers, and pediatric/AYA patients.
“We have to educate families on what a clinical trial is. A lot of times, when a parent hears the word ‘trial’, they think it’s experimental. It’s really looking at what can give you the best quality of life and event-free survival,” says Lori Ranney, DNP, APRN, CPNP, CPHON, Children’s Minnesota, a nurse practitioner. “We look at the family as a whole, and if it’s appropriate, involve children and AYA populations in the discussion.”
Hospitals and other treatment facilities may also include their child-family-life interdisciplinary teams and social workers to provide additional support and resources.
Children’s Minnesota is a large pediatric oncology institution that also has a well-known referral center. About 90% of eligible patients are treated through participation in clinical trials. Children’s Minnesota works to partner with the four surrounding states – Wisconsin, North Dakota, South Dakota, and Iowa – with the goal of bringing care closer to home for patients.
“The RACE for Children Act is updated legislation that went into effect in the summer of 2020. It specifically targets pediatric cancer. The intent is to get more cancer drugs studied in children, thereby ultimately getting new and improved and aid-proof drugs to the children,” says Missy. The RACE for Children Act expands prior legislation and policies designed to increase the development of pediatric drugs, treatments and therapies and eliminates the orphan exemption for pediatric studies for cancer drugs directed at relevant molecular targets (1).
One way to provide medications and treatments to children, particularly in a rare disease space, where there is a limited number of patients, is to consider that some adolescents may be able to receive similar dosages that adults receive, particularly older adolescents, due to their underlying organ maturation. Taking a patient’s physical maturation into account allows for more adolescents to participate in clinical research, even if they are not yet 18 years old. Minor children (under the age of 18 years old) cannot legally provide informed consent to participate in clinical research. They are asked to provide “assent” or “dissent”, meaning they agree or do not agree to take part. To participate in this process, the child must be mature enough to understand the trial and what it entails. (2)
Children’s Minnesota’s AYA Center tailors care to adolescent’s and young adults’ distinct needs, which can significantly impact outcomes. “We strive to make our AYAs feel individualized,” explains Lori. “We have formed a team of physicians, nurse practitioners, and nurses that focus on AYA patients and their individual needs. The AYA population is a unique one. We want to make sure we are helping them gain independence, by looking at what is important to them, such as friends, school and socialization. We have also formed an AYA support group, where patients go out and do fun activities together, so they can see that there are other people living like them, that can connect to in ways that they can’t necessarily connect to their other friends.”
You can learn more by accessing the webinar recording here. View CISCRP’s library of webinars and podcasts here.
To search for medical conditions in a specific location, visit our Search Clinical Trials page.
To stay informed about clinical trials, visit our Resources page.
(2) https://www.cancer.gov/about-cancer/treatment/clinical-trials/patient-safety/childrens-assent
Authored by Melissa E. Daley, Communications & Marketing Manager, CISCRP
CISCRP hosted a 3-part webinar series titled “Navigating Rare Disease and Clinical Research: Every Patient Matters”. This article brief is based on the first episode, “Rare Disease Clinical Trials: Being Informed”. Moderated by Christian Rubio of Global Genes, panelists included Dr. Jahannaz Dastgir of Goreyeb Children’s Hospital of Morristown, New Jersey, Melanie Havert of Rare Patient Voice, Jenn McNary, Founder of One Rare, and Stephanie Loomer, Project Manager, CISCRP. You can access the webinar recording here.

The biggest difference between common disease and rare disease clinical trials is “…probably the amount of people that can be enrolled in the trial,” says Dr. Jahannaz Dastgir, Director of Clinical Research, Applied Therapeutics and Lead Physician at Atlantic Health System’s Pediatric Neuromuscular Program. “With conditions like diabetes or heart disease, for example, you could have very large numbers of patients. In rare diseases, you would have a much smaller number, because there might be 20 cases of the condition, worldwide. You have to work out the statistics to make sure you have the right amount of data over the right amount of time to get the study to be statistically significant so that the drug can be approved.”
A disease or condition is classified as “rare” in the United States if it affects less than 200,000 individuals. This definition varies in other parts of the world. For example, in the European Union, a disease is defined as “rare” when less than 1 in 2,000 individuals are impacted. While there is no exact count, it’s estimated that there are approximately 7,000 rare disease effecting 25 to 30 million Americans (1) and over 300 million children and adults globally, roughly 3.5% to 5.9% of the population (2). Conducting clinical studies in the rare disease space to find safe and effective solutions is a collaborative effort by stakeholders in the clinical research enterprise including patients, patient advocates, product developers and medical research professionals.
“Our clinical trial journey really started with me having no knowledge of clinical trials,” recalls Jennifer McNary, a mother of four, rare disease patient advocate, educator and founder of One Rare, a nonprofit organization whose mission is to improve experiences for the rare disease community through education, mentoring and peer support. Jennifer’s connection to the rare disease community is particularly poignant.
“My three sons all live with rare diseases. My first two sons, are now 22 and 19, are living with Duchenne Muscular Dystrophy. I also have a third son living with 2 rare diseases, primary immune deficiency and congenital cholesteatoma. He is 13 years old. And I have a daughter who is healthy,” says Jennifer. When her two older sons were diagnosed as children, Jennifer was advised that “…there were no treatments, no therapies, there was nothing I could do and in fact, there were no clinical trials that we could think about enrolling in.” Jennifer took matters into her own hands and shares “I spent a lot of years raising money and funds for science and going to advocacy meetings.”
Jennifer also pursued clinical research as a healthcare option for her two older sons in hopes of changing the trajectory of their disease progression.
“Thankfully, when Max was 9 years old, and his brother, Austin was 12, we were allowed to participate in our first clinical trial. It was a lot of work to get to this point,” she recalls. Through personal connections, Jennifer learned about a clinical trial in Columbus, Ohio, at Nationwide Children’s Hospital. The clinical study was specific to a certain mutation in Duchenne Muscular Dystrophy.

“I dug out my kids’ genetic report and I realized that my kids actually had this genetic mutation and could qualify for the study. When I called the (clinical research) site and asked them if my sons could be part of the study, they told me that there were a few things we had to do. The first thing was that we had to answer a few questions about the kids’ mobility and ability to walk. Unfortunately, because Austin was 12 and had lost the ability to walk at age 10, he was not able to enter the study or even be considered. But Max was the right age, has the right genetic mutation, and he was functionally the right kind of kid that they were looking for to bring into this 12-person study. And so, I packed up Max, and my newborn daughter at the time, Nora, and I left my three-year-old son and my 12-year-old non-ambulant son with some family and friends and we flew to Columbus, Ohio to meet with the doctors running the study,” says Jennifer.
At the time, Jennifer and her family lived in Vermont. Weekly travel to the clinical research center was required. “I didn’t have a lot of money and a lot of patients do not have the money to fly weekly, stay in hotels, get rental cars, so I wanted to make sure that this was all going to be reimbursed and that patients were not going to have to pay for their time in a study,” says Jennifer.
It’s important to ask questions about all aspects of the clinical study, so that you have a complete understanding of what it entails for both the participants and caregivers. Equally important, is that you feel comfortable and confident in asking questions to the research center staff- study coordinators and/or the Principal Investigator.
“One of the questions I asked when we were evaluating this study was what happens at the end of the study, if my child didn’t get the drug, do they continue to receive the study drug, (when the study is completed)? This is called an extension study. I always ask at the beginning of a clinical trial, is there an extension planned, and will all of these patients receive the active drug, if it works?” says Jennifer.
Melanie Havert is a patient advocate and project manager at Rare Patient Voice, which provides patients and caregivers with rare diseases an opportunity to voice their opinions through surveys and interviews to improve medical products and services. When she is discussing details with clinical research staff “A question I always like to ask is have any other people had this drug yet or are we going to be the first ones to try this? Of course, it’s tested extensively before it gets to people, but I like to know where we’re at, at that phase.”
“My instinct is to ask questions about the data that exists around this and why do they (clinical research staff) think it’s going to work. What do you know about this therapy that leads you to believe that it’s going to do something?” says Jennifer. She also advises that participants or caregivers need to ask about any lasting implications from participating in the study. “Ask that question because you don’t want to end up eliminating yourself from future clinical trials and from having flexibility to choose what therapies you want to take. Once you’re in a clinical trial, you often can’t change your current treatments.”
A common question that participants and caregivers ask is what the first day of a clinical trial is like.
“The first day can be pretty intense,” says Melanie. “In my experience, you get a stack of papers, and someone sits down with you and you spend a couple hours going over these papers, and they make sure that you completely understand what you’re about to do to participate in the clinical trial. They really walk you through the process.” (This is called Informed Consent and you can learn more about it here). There may also be blood draws and urine samples taken, along with other initial benchmark testing. “It really depends on the specific drug and how they are handling it that day. It’s pretty intense but it’s worth it.”
Dr. Dastgir adds “You will get additional testing that is part of the trial. And the results of these you may or may not be privy to. It’s really important to maintain the standard of care locally.” Dr. Dastgir says the care that a participant receives during a clinical study is “…an enhancement of care, better access to experts but not a substitution for the standard of care that you get back home with your local provider.”
Melanie observes that “Something that I’ve noticed is that when you go see your regular doctor, you can ask them questions and they have answers for you. When you’re in a clinical trial, it’s the doctors that are asking you questions, and you’re giving them the answers.” Participants can ask questions in a clinical trial, as well.
In the era of social media, patients and caregivers have unprecedented access to information sharing platforms. Dr. Dastgir says “Social media is the Wild Wild West in terms of what kind of information you’re receiving, and whether it’s correct or not. When people sign the consent form, there’s some level of discretion and confidentiality that exists, and whether or not that gets implemented is primarily good faith.”
Both common disease and rare disease clinical trials for children and adults are monitored by the FDA (Food and Drug Administration) the NIH (National Institute of Health) and IRBs (Institutional Review Boards). You can learn more about safety protocols in clinical research here.
“I do have a lot of faith in the safety of this system,” says Jennifer. “There are a lot of safety nets to capture adverse events and to protect children in studies. I am happy to report that this was a positive example of being in a clinical trial, because this therapy was approved based on the study that Max was in. We’re still on the hunt for the next best therapy, and we’re hoping to be accepted into another trial. I would give this experience a 10 out of 10.”
“Most rare diseases are genetic or have a genetic component and 75% of rare diseases are without a single FDA-approved treatment. On average, it takes an average of 7.3 years to receive an accurate diagnosis of a rare disease,” says Christian Rubio of Global Genes. Clinical research is essential to addressing these disease states and indications in order to find treatments, therapies and cures.
You can view part-two of the series, “Rare Disease Clinical Trials: How to Prepare for When the Clinical Trial Ends” here and part-three, “Rare Disease Clinical Trials: After Participation, Paying It Forward” here.
To search for medical conditions in a specific location, visit our Search Clinical Trials page.
Access the companion infographics:
To stay informed about clinical trials, visit our Resources page.
Sources
(1) https://rarediseases.info.nih.gov/diseases/pages/31/faqs-about-rare-diseases
(2) https://www.rarediseaseday.org/article/what-is-a-rare-disease
###
The Trifecta lived daily by Rare Disease families is now experienced by the whole world: 1) Isolation, 2) Medical Uncertainty, 3) Disruptions in Home/Work Life. Scott Schliebner of ICON & Cristol Barrett O’Loughlin of Angel Aid Cares discuss how caregivers are navigating the impact of these three forces for the whole family.
You can access the article brief based on the webinar here.

Moderator
Scott Schliebner
SVP, Scientific Affairs
Therapeutic Expertise Head
Center for Rare Diseases, ICON
Click on image for biography.

Panelist
Cristol Barrett O’Loughlin
Founder & CEO
Angel Aid Cares
Click on image for biography.

Gain a better understanding of rare disease clinical trials by listening to patient advocates and health care providers, learn how to be prepared for when the trial ends, and hear from those who chose to be advocates in this 3 part webinar series.




Moderator
Christian Rubio
VP of Strategic Advancement,
Global Genes

Panelist
Dr. Jahannaz Dastgir DO
Director, Pediatric Neuromuscular Program,
Goryeb Children’s Hospital

Panelist
Melanie Havert
Project Manager,
Rare Patient Voice, LLC

Panelist
Jenn McNary
Founder & Patient Advocate,
One Rare

Presenter
Stephanie Loomer
Project Manager,
CISCRP

Marsha Lanes,
Genetic Counselor/
Medical Editor,
NORD

Dr. Tracy Dixon-Salazar,
Executive Director,
Lennox-Gastaut
Syndrome Foundation

Richie Kahn, MPH
Senior Director,
Patient Engagement,
Medable Inc.

Dana Holinka,
Operating Board Member,
TSC Alliance

Britta Dornan
EveryLife Foundation for Rare Diseases

Ryan Colburn
Patient Advocate
(Pompe disease)

Dr. Kim Stephens
Project Alive

Marc Yale
International Pemphigus & Pemphigoid Foundation
Part 1:
Part 2:
Part 3:
I graduated with my master’s in medical anthropology from Boston University School of Medicine in 2016. Prior to starting at CISCRP, I worked on research studies focused on patient experiences with health care. Most recently, I worked on several projects related to substance use and people living with HIV. I am incredibly passionate about working with vulnerable populations and increasing access to care for patients through research. As Project Manager in Research Services, I am excited to connect with new patient groups and make research more approachable for vulnerable populations.


Dominantly Inherited Alzheimer’s Disease Brochure
Expanded Registry Flyer (English)
Enfermedad de Alzheimer de herencia dominante
Expanded Registry Flyer (Spanish)
Forgetting the Little Things
Concerned About Memory Loss?




Click on the resources listed below to view the full versions of LCI’s materials.


Krysal Doucet has worked in Research as a CRC for 11 years and as an Associate Site Director for 2 years. She started her path in the health care industry by becoming a C-MA. After completing the Medical Assisting course, she was introduced to a great opportunity working as a Clinical Research Coordinator with Benchmark Research.

Missy Hansen MSN, APRN, CPNP, CPHON, joined ICON in 2019 as a pediatric strategy liaison. She has 25+ years of experience as a pediatric nurse practitioner, including 17+ years in pediatric hematology/oncology at Children’s Minnesota, the largest hematology/oncology service line in the region, providing care for infants through young adults diagnosed with hematologic and/or oncology conditions. Ms. Hansen gained expertise working in inpatient, outpatient, and urgent care type settings. Ms. Hansen has in-depth experience working with the Children’s Oncology Group—the largest consortium with the most open pediatric studies around the world. She also has experience working with other consortia that conduct trials for pediatric to young adult patients.
Lori Ranney DNP, APRN, CPNP, CPHON has worked in pediatric oncology for 20 years and has been a PNP at Children’s Minnesota for over 13 years. She has a special interest in leukemia/lymphoma, patient/family education, AYA population, and oncofertility. She is a member of the Children’s Oncology Group and has actively enrolled patients in clinical trials for over 15 years.
Mark has over 20 years of experience in the pharmaceutical and biotech industries and currently leads ICON’s global pediatric center of excellence. Having earned his medical degree and master’s degree in clinical nutrition from the Chicago Medical School, Dr. Sorrentino completed both a residency in pediatrics and a fellowship in pediatric critical care at Children’s National Medical Center (CNMC) in Washington, DC. Currently, Dr. Sorrentino holds an appointment as an assistant clinical professor at the George Washington University School of Medicine. Prior to joining the industry, Dr. Sorrentino was an attending physician in the CNMC pediatric intensive care unit for 8 years and participated in numerous industry-sponsored critical care trials. He holds active medical licenses in California and Maryland.
Based in Minnesota, Dr. Perkins has 21 years of experience in clinical research across Phases I–III with a focus on hematologic malignancies. Before joining ICON in 2018, she was in clinical practice for 15 years specializing in leukemias, lymphomas, and long-term complications of cancer therapy. Dr. Perkins has supported multiple oncology/hematology trials across indications and phases. She is board certified in pediatrics and pediatric hematology and oncology and holds a master’s degree in clinical research.

Christian oversees the development of new strategic partnerships, products and services to help shorten the diagnostic odyssey, improved access to research and help expand the number of treatments available for all rare disease patients and caregivers.

Dr. Dastgir specializes in pediatric neurology and is the director of the pediatric neuromuscular medicine program at Goryeb Children’s Hospital in Morristown, NJ. Her current practice is primarily composed of patients with rare disorders.
Dr. Dastgir also has experience in being an investigator for clinical trials involving such rare conditions as spinal muscular atrophy, duchenne muscular dystrophy, and infantile neuroaxonal dystrophy.

Generally, chronic health conditions greatly impact the lives of those within a household, not just the patient, but also the caregiver(s) and other members of the family; because of this, Mel has made it her mission to rise above the health obstacles within her own family and help others gain the knowledge and confidence to do the same. Having a chronic condition does not define a person, while it may affect the quality of one’s life, it does not need to become an unsurpassable obstacle preventing one from exploring their dreams and living life to the fullest.
Mel loves speaking publicly and jumps at every opportunity to do so, she has spoken at schools, rallies, congregations and even at the California State Capitol; no audience is too big or too small. She is passionate about helping people gain confidence in themselves, to learn self-advocacy, to find their voice and gain the inner strength to effectively be heard, and to live life to its absolute fullest potential.

Jenn McNary is a trusted voice in the rare disease community, as a mother, public speaker and fierce advocate. Her work in the rare disease space as a thought leader earned her the Ryan’s Quest Ryan’s Hero award in 2013, a nomination for the Global Genes Champion of Hope award in 2014, and the prestigious 2017 Meyer- Whalley instrument of change award. Formerly as the director of outreach and advocacy at a Massachusetts based non-profit foundation, she was responsible for the organization of the largest FDA advisory committee hearing in history, with over 1000 duchenne advocates, families, clinicians and researchers in attendance.
Jenn has unique experience in the drug development field, as a parent of children enrolled in the clinical trials, an advocate engaging with the regulators and as a consultant helping to develop programing for patients. Currently, Jenn is consulting in the biotechnology space with an expertise in caregiver/patient engagement, including bringing the patient voice to drug development and solving barriers to access.
Her other activities include serving as the Founder of One Rare, a non-profit formed to meet the needs of young adults with rare and chronic conditions and raising her four children in Massachusetts.

Mr. Schliebner is a clinical development executive with a 25-year background focused on rare diseases, innovation, and patient-focused approaches to drug development. He is passionate about reducing the burden of clinical trial participation and leveraging novel approaches and technologies to bring new therapies to patients faster. Mr. Schliebner also serves as the Co-Chair of Global Genes’ Corporate Alliance, serves on the Board of Directors for Uplifting Athletes, and supports several rare disease panels and committees. He holds a Master’s Degree in Public Health (MPH) from the University of Utah School of Medicine, and completed a Graduate Research Fellowship at The National Institutes of Health.

Cristol Barrett O’Loughlin is a seasoned executive and storyteller. As Founder and CEO of Angel Aid Cares, Cristol is fiercely passionate about providing social, emotional, physical and financial relief to mothers of children with rare disease. A former UCLA instructor, she co-founded the advertising firm, The Craftsman Agency, and is humbled to advise global brands; NBA, Disney, Fox, Cisco Systems and Google. During her tenure at IBM Life Sciences, she helped accelerate advancements in cheminformatics and biotechnology. She presented a TEDx talk “Caring for the Caregivers: 3 Tools for Self-Care”.

Rosamund Round leads Parexel’s Patient Innovation Center, focused on improving research access and experiences for patients and caregivers. This includes leadership of the decentralized clinical trials service, activities to improve diversity in clinical research, and creation of other tools and services that reduce practical, financial and geographical barriers to participation.
She has 17 years of leadership experience in patient engagement and innovation roles, and regularly presents and authors articles on the topic.

Liam Paschall is a transgender man who has found immense courage, power, and pride in accepting the truth of who he is. His pronouns are he and him.
He is an entrepreneur, public speaker, and facilitator, with a lifelong goal of changing hearts and minds – one person at a time. He is a passionate servant to the LGBTQIA+ community with the ability to motivate and inspire others to live out loud.
Having started his female to male transition at the beginning of last year, Liam knows first-hand how critical and life-altering inclusive healthcare and clinical trials can be to members of the LGBTQIA+ community.

Dr. Sebastian Barr is a licensed psychologist currently based in Western Massachusetts. He received his PhD in Counseling Psychology and completed advanced training in health service psychology and psychotherapy research at Cambridge Health Alliance under the auspices of Harvard Medical School. His scholarship centers on the experiences, mental health, and mental healthcare needs of members of the trans community, with a particular recent focus on the impacts of bias and non-affirmation. His research has been recognized nationally and internationally and published and cited across multiple journals and textbooks. Additionally, he specializes in helping institutions and healthcare providers adopt affirming, inclusive, and evidence-based practices in both clinical work and research with members of the trans community. He is a proud transgender man and incorporates personal lived and community experience into his work.
For over a decade, Adam has conducted clinical trials across multiple therapeutic areas as a research coordinator, monitor, project manager, and director at various types of organizations—investigational sites, CROs, academia, pharma, and tech. He received a master’s in clinical research from The George Washington University. In June 2020, he joined as Director of Clinical Operations at Curebase, a provider of software and services purpose-built for decentralized clinical trials (DCTs), where he is responsible for oversight of DCT services.

Arsheen Ali is a Project Manager and has served in this role with Curebase for over two years. In this capacity, she manages multiple decentralized clinical trials. Her background includes a variety of healthcare and research experience. She received her bachelor’s in integrative biology from UC Berkeley. Arsheen’s main interests are public health (population and community health focus), increasing healthcare quality and access (especially for minority/marginalized populations), and maximizing the efficiency of research.

Myra Lane is Lead Virtual Research Coordinator at Curebase with over three years of clinical research experience in the decentralized clinical trial space interacting directly with patients. She has worked in various therapeutic areas including neurology, dermatology, and oncology. She is passionate about the impact that the digital therapeutics approach has on addressing unmet patient needs by providing universal access to clinical research and accelerating the development of treatments.

Ken Getz is the founder of CISCRP and chairs the board of directors. He is also a professor and the Director of the Center for the Study of Drug Development, Tufts University School of Medicine where he conducts grant-funded studies on pharmaceutical R&D management and execution; protocol design optimization; contract service provider and investigative site management; e-clinical technology and data usage; and patient engagement. Ken is the founder of CenterWatch, a leading publisher in the clinical trials industry and one of several companies that he has created and sold. A well-known speaker at conferences, symposia, universities and corporations, Ken has published numerous articles and chapters in peer-review journals, books, and in the trade press. He is the author of two nationally recognized books for patients and their advocates including The Gift of Participation, and the recipient of several awards for innovation and scholarship. Ken has held a number of board appointments in the private and public sectors, including serving on Otsuka’s Patient Assistance Foundation, the Institute of Medicine’s Clinical Research Roundtable, the DIA Foundation, the Consortium to Examine Clinical Research Ethics, and the Clinical Trials Transformation Initiative.

At CISCRP, I manage the design, implementation, analysis and reporting of a variety of CISCRP research studies. I have more than 15 years of experience conducting primary and secondary research studies in the healthcare, life sciences and consumer goods industries. Prior to CISCRP, I worked at Colgate-Palmolive as a research manager. I hold an MBA from the Graduate School of Management at Boston University and a Bachelor of Science degree from Bryant University. I am passionate about helping others, and CISCRP offers ample opportunities in that regard. People often comment that I am a nice and genuine person. And I think those characteristics help me connect to the patients I interact with regularly through my work. I especially enjoy being involved in bringing patients and clinical operation teams together through the CISCRP Patient Advisory Boards; speaking with each other about ways to make clinical trials a better experience overall is very rewarding for me.

As a Peace Corps Volunteer, I served as an English Literacy Facilitator in the Kingdom of Tonga. There, I gained invaluable experience working alongside my community and counterparts through projects such as student-centered learning initiatives within the classroom, grant writing for better access to technology, establishing a school library, as well as promoting girl’s empowerment and opportunities for fitness and healthy living. Throughout my service, my favorite experiences were always connecting with individuals in the community – exchanging stories, cultures, traditions, and laughter. Additionally, I am a graduate of Connecticut College where I earned a B.A. in Psychology and an Elementary Education certification. I am excited to have the opportunity to apply my love of education, psychology, and research through my work at CISCRP. As a Project Manager, I enjoy working with a variety of individuals from diverse backgrounds and experiences to help amplify the patient voice within clinical research trials.

I graduated with a B.A. in Sociology from Skidmore College in May 2020. At Skidmore, I worked on multiple research projects including a journal article I co-authored with a professor focusing on Tor and the Dark Web, as well as my Senior Thesis, which examines the relationships between mental health and access to natural environments. Through my research projects, as well as my education in Sociology, I learned the importance of using research to improve access to crucial resources and institutions that help communities grow and thrive. I also had the opportunity to intern for Habitat for Humanity, which strengthened my interest in working for a non-profit organization that aims to overcome barriers in the way of essential resources such as housing or healthcare information. I am excited to use my research experience and my love for working with people to help improve the clinical research process, and highlight the patient experience as central to the development of clinical trials.

Kim Harper, began her clinical research experience as a Clinical Research Coordinator back in 2007. Over the next 7 years she worked as a CRC gaining experience working for an arthritis clinic and a research center. In 2014, Ms. Harper was brought on by Benchmark Research, a leading clinical research firm as a CCRC. She quickly worked her way through the ranks to Assistant Site Director and in 2020 Kim became promoted to Site Director.
During her 14 years in the field, Kim has been a significant contributor to the studies she has worked on which include Phase 1-4 treatment, preventative and diagnostic trials on pediatric, adult, and elderly subjects. Kim has diverse experience in vaccine, drug, and device trials as examples therapeutic areas she has worked on include ebola, anthrax, COVID-19, diabetes, influenza, meningococcal, antipsychotics, depression, alzheimer’s disease, osteoarthritis, and more. During the COVID-19 pandemic, Kim thrived in the high pressure environment and led her North Shore New Orleans research site to successfully conduct 2 coronavirus studies including a high profile vaccine. Kim is known amongst her peers for her proven ability to reach across personal and professional barriers to expedite effective health care.

Stephanie is a patient advocate at The Young Face of Arthritis.

As a rare disease patient living with primary lymphedema (LE) for over three decades, Britta remains determined to challenge her limits rather than to let LE limit her challenges. Despite wearing compression garments 24 hours a day, she has skied Mount Tremblant, completed the 10k Chesapeake Bay Bridge Run, and climbed the Great Wall of China. Britta pays it forward by sharing “advice, comfort, and positive thinking” on her award-winning blog, lymphedemadiary.com. As Senior Director of Communications and Marketing for the EveryLife Foundation for Rare Diseases, Britta initiates strategies that inspire patients and caregivers to engage in advocacy and make their voices heard. Britta lives in Arlington, Virginia with her husband and two very spoiled cats.

Ryan Colburn is a guy with 2(+) typos on his GAA gene on chromosome 17. He has a professional background in engineering and operations management; spending portions of his career working on race cars, airplanes, and rockets. Diagnosed with Pompe disease in 2015, he has spent the time since learning about rare disease topics including research, advocacy, and development of treatments to better understand how to participate in the rare disease ecosystem. He is passionate about patient empowerment and engagement; actively developing relationships with other patients, advocacy groups, researchers, and pharmaceutical companies. He is driven to improve the health of the rare disease ecosystem by shifting the view from patients as “subjects” to one of participants, collaborators and partners who help find the most effective ways to tackle the challenges of rare disease and break down barriers to the acceleration of progress. Ryan has participated in nine clinical studies since he was diagnosed, and has shared his perspectives with industry and advocacy organizations to improve the patient experience within the clinical research space.

Dr. Kim Stephens is the president of Project Alive, a nonprofit organization dedicated to research and advocacy for Hunter syndrome. Project Alive that is a powerful voice for children and adults with Hunter syndrome and brings together families and advocates with researchers, industry, and regulators. Having a son with Hunter syndrome herself, this is also a personal mission for Kim. Her son Cole has been participating in a clinical trial for the past 6+ years. Having gone through the ups and downs of clinical trial life, Kim is a strong advocate for creating better outcome measures, integrating the patient voice in trial design, and considering the entire cycle of the clinical trial – from the patient’s doorstep to the clinic and back home again. She frequently speaks as a rare disease advocate at conferences and events and serves as a mentor and resource for newly-diagnosed families.
Kim is also the founder of Inclusive Thinking – a consulting company dedicated to increasing diversity and inclusion through research, education, and strategic planning. Before founding Inclusive Thinking, she had a twenty-year career with IBM, most recently as the Global Diversity & Inclusion Communication and Education Lead. She has spoken at conferences around the world and conducted workshops on unconscious bias, cultural awareness, women’s leadership, accessibility, and other topics.
Kim earned her doctorate in Business from Georgia State University and focused her dissertation on implicit bias and the role of transformational conversation and social identity on behavioral change.

Marc Yale was diagnosed in 2007 with Cicatricial Pemphigoid, a rare autoimmune blistering skin disease. Like others with a rare disease, he experienced delays in diagnosis and difficulty finding a knowledgeable physician. Eventually, Marc lost the vision in his left eye from the disease. This inspired him to help others with the disease. In 2008, he joined the International Pemphigus and Pemphigoid Foundation (IPPF) as a Peer Health Coach. He worked with people to improve their quality of life and encouraged them to become self-advocates. In 2009, he helped develop the Pemphigus and Pemphigoid Comprehensive Disease Profile giving experts insight into the patient perspective. In 2016, Marc became the Executive Director of the IPPF. He has recently become the Advocacy & Research Coordinator of the IPPF so that he can focus on research and advocate for all of those affected by pemphigus and pemphigoid. He is a member of the American Academy of Dermatology Drug Transparency Task Force, sits on the Executive Board of Directors for The International Alliance for Dermatological Patient Organizations as their Treasurer, serves on the Board of Directors of Haystack Project, and is a committee advisor for Rare Disease Legislative Advocates. Marc recently joined Rare Disease International in the establishment of the WHO Collaborative Global Network for Rare Diseases Panel of Experts to ensure a lasting impact on the lives of people living with a rare disease around the globe.
Marc currently resides in Ventura, California with his wife of 31 years.

Mike Wenger is Global head of Patient Engagement at Informa Pharma Intelligence. As both a patient and software developer, Mike is passionate about patient access to clinical trials. He is spearheading Citeline Connect, the only end-to-end platform for clinical trial education, recruitment and enrollment, enabling sponsors to accelerate study startup and boost engagement. Mike was named one of the 2020 PM360 ELITE 100 in the Patient Advocates category and a 2020 Force for Change Illuminator. He also was a finalist in the Patient Advocate of the Year category in the 2020 Medigy HITMC Awards.

Wes Michael founded Rare Patient Voice in 2013 to give patients and caregivers with rare diseases the opportunity to voice their opinions in research studies. Rare Patient Voice has now conducted thousands of studies and rewarded patients and caregivers with over $8 million for their participation. Many have been recruited in person by Wes and his team at patient events like fund-raising walks and patient conferences, and through a referral program with patient advocacy and support groups. Rare Patient Voice now covers non-rare as well as rare diseases and conditions and has expanded from the United States to Canada, the United Kingdom, France, Germany, Italy, Spain, Australia, and New Zealand.
Before launching Rare Patient Voice, Wes worked for healthcare market research firm Kantar Health. He previously was a brand manager and market research manager at McCormick (the spice company) and General Mills (working on Wheaties, Total and Kix cereals). He has a BA from the University of Pennsylvania (with a year at Edinburgh University) and an MBA from the University of Chicago. Wes was recently inducted into the DTC National Hall of Fame, honoring individuals who have demonstrated extraordinary achievement in the advancement of direct-to-consumer marketing.

Steve Jones, is President of EU-IPFF, the European Idiopathic Pulmonary Fibrosis and Related Disorders Federation and part of the Citeline Connect referral collective. EU-IPFF is dedicated to making clinical trials work better for patients in partnership with pharma and regulators in UK and Europe. Steve also is chair of trustees of the UK patient organization Action for Pulmonary Fibrosis and a council member for the European Lung Foundation. He also sits on the steering committees of four major non-pharma clinical trials funded by the UK’s National Institute of Health Research. Steve himself is a pulmonary fibrosis patient and had a lung transplant five years ago.

Ashley Smock is a woman living with ovarian cancer. She took part in the Rare Patient Voice/Informa survey on patients and clinical trial participation in 2021.

Amy brings a comprehensive understanding of drug discovery and drug development from the research laboratory to patients’ bedside from 20+ years of experience in academic institutions, biotech companies, and CROs. Originally trained as a molecular biologist, she transitioned into drug development and came up through clinical operations before joining the Center for Rare Diseases in 2017. She has contributed to discovery and development of treatments for many rare disease patient communities, from rare cancers to rare neurodegenerative disorders, including development of a gene therapy treatment now commercially available to rare disease patients.
Amy leads the Gene Therapy Think Tank and is a Subject Matter Expert in the Center for Immuno-Oncology, Cellular, and Gene Therapy. She provides full life cycle support for gene therapy programs outside of oncology, from study design through study close out. This includes close collaboration with sponsor teams, study physicians, clinical operations throughout the program, as well as supporting integration of patient partnership into clinical operations. She is passionate about enhancing the efficiency of clinical trials through cooperative productivity and patient-centered design – key elements of “Market Aware” clinical development protocols, and a proven pathway to commercial success.

Laura Iliescu, MSc, has 20 years of experience in development and commercialization of therapies, and patient-centered healthcare services. She has held strategic development roles in rare and complex conditions in leading pharmaceutical, biotechnology, CRO and clinical homecare organizations. Her varied experience comprises strategic development throughout every phase of the product lifecycle from pre-clinical to beyond patent expiry in North America and Europe. She has deep experience in rare metabolic, rare neuromuscular an rare respiratory indications among others.
Her background in human factors engineering and user-centered service design methods informs her passion for patient-centered development and for evolving the clinical development paradigm around patients as key stakeholders.
In her current role within ICON’s Center for Rare Diseases, Laura advises product development companies on patient-centered clinical strategy to optimize both study efficiency and the experience of rare disease patients and caregivers. She leads the Center’s Patient Advocacy Strategy team, who support collaboration between companies and rare disease Patient Advocacy Organizations through study design and conduct.
Laura grew up in Toronto, Canada, after which her career (and love of travel) have taken her to more than 40 countries in North America, Europe and Asia. She currently lives in Toronto, Canada with her partner and has both family and friends who are affected by rare conditions. Laura holds a Masters of Human Factors and Ergonomics from the University of Nottingham.

Kelli Wright is the Senior Manager of Patient Advocacy for Harmony Biosciences working to keep Patients at the Heart of everything we do at Harmony. It’s critical to include the patient voice in drug development efforts and Kelli is honored work with patient communities, people living with rare neurological diseases, caregivers, and patient advocacy organizations to share their lived experiences across functions at Harmony.
With a 15+ year non-profit career, Kelli has a deep understanding of the patient needs and experiences. Most recently Kelli was the National Director of Strategic Initiatives for CureSearch for Children’s Cancer, driving the strategic program of CureSearch by staying in tune with the barriers in drug development. Kelli learned from innovators in the industry, academic and regulatory space, as well as patients and disease-foundations, to address obstacles and develop action plans to close the communication gaps and reduce duplication of efforts.

Kendall is a driven health advocacy professional with strong community outreach, patient association, health care provider, rare disease and chronic illness expertise. She specializes in patient advocacy throughout rare disease clinical drug development. She currently serves as the Patient Advocacy Lead, Early Development , at Spark Therapeutics. In this role she supports Sparks preclinical and early clinical development programs. Previously, Kendall served as a Patient Advocacy Strategy Lead at PRA Health Sciences and as the Director of Strategic Alliances at Global Genes, a leading rare disease patient advocacy organization. She has held key roles in patient advocacy and patient education in both the nonprofit and biopharmaceutical industries. Kendall’s passion is to improve the health outcomes of individuals living with rare diseases while integrating advocacy strategy into clinical drug development. Kendall specializes in cultivating partnerships with patient advocacy organizations, identifying and partnering with Key Opinion and Community Leaders, identifying business needs, developing customized programs to achieve key outcomes and balancing a global focus with national, regional and local patient centric partnerships. Kendall works with leaders in the rare disease nonprofit community & biotechnology space to advance progress in rare disease drug development. Kendall also serves on the board of directors of Team Telomere and as a strategic advisor to the Rare and Undiagnosed Network. She holds a Master’s Degree of Public Health from Michigan State University as well as a Bachelor’s of Science in Psychology from Loyola University, Chicago. Kendall currently lives in Pittsburgh, PA with her husband, son and dachshund.

Sarah Nechama Frisch is a woman living with narcolepsy with cataplexy. She took part in the Rare Patient Voice/Informa survey on patients and clinical trial participation in 2021.

Julie Holtzople is Senior Director, Clinical Transparency and Data Sharing, AstraZeneca.
Christopher Pfitzer is Associate Director, Transparency Operations Lead at UCB Biosciences, Inc.






{kind=link}
{kind=link}