



Rosamund Round, Vice President, Patient Innovation Center & Decentralized Trials, Parexel International, Liam Paschall, Global Training Business Partner, Parexel International and Dr. Sebastian Barr, PhD, Licensed Psychologist & Consultant, discuss the barriers that transgender and non-binary individuals face to medical care and ways to scale access to clinical research participation.
Related Articles:
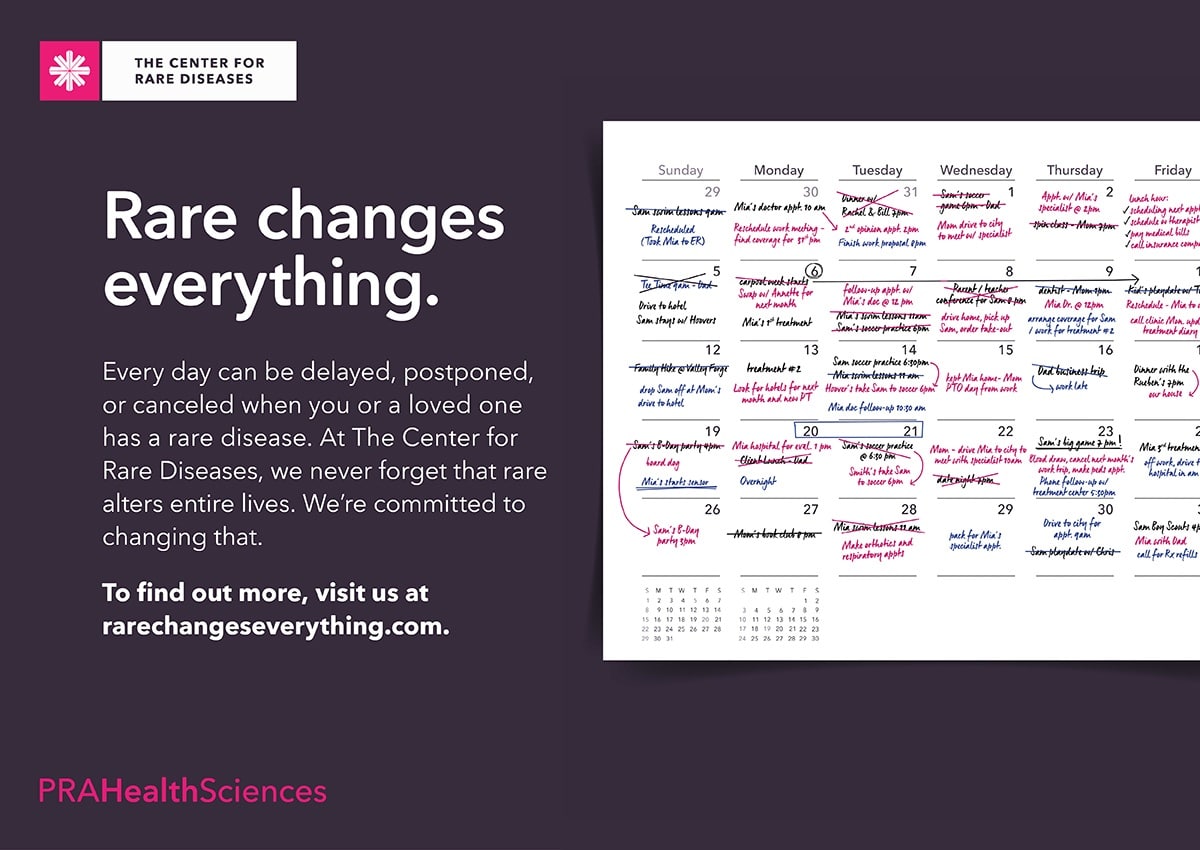
Working Towards A More Inclusive Environment: Transgender & Non-Binary Participants in Clinical Research
Improving Access to & Experiences of Transgender & Non-Binary Patients in Clinical Research
Rosamund Round, Vice President, Patient Innovation Center & Decentralized Trials, Parexel International
Click Photo to Read Bio
Liam Paschall, Global Training Business Partner, Parexel International
Click Photo to Read Bio
Dr. Sebastian Barr, PhD, Licensed Psychologist & Consultant
Click Photo to Read Bio
Authored by: Melissa E. Daley, Communications & Marketing Manager, CISCRP
The advent of the COVID-19 pandemic has scaled public interest in clinical research, and has increased the implementation of DCTs, decentralized clinical trials. SMEs from Curebase, a software and services provider specializing in DCTs, shared what DCTs are, how they work and differ from the traditional model of clinical conduct, and the importance of diverse participation in a 15-minute Flash Webinar. Arsheen Ali, Clinical Project Manager, began by outlining the conventional approach to clinical trials.
“Traditionally, clinical research activity occurs in person, at a designated physical location, which is generally referred to as a research site,” explains Arsheen. “A doctor, called a PI or Physician Investigator, along with other clinical research staff including nurses and clinical research coordinators, facilitate participant care and the collection of data around the clinical study so that the data can be analyzed.” Participating in a clinical study introduces many moving parts for patients and caregivers, including issues around travel to and from the study center, taking time off from work, coordinating childcare and other personal impacts.
To gain better understanding of how DCTs provide an added level of convenience for participants, Myra Lane, Lead Virtual Research Coordinator shared that
“Decentralized clinical trials help promote a more patient-centric approach, addressing participants needs that go unmet in traditional clinical trial models. DCTs typically incorporate the use of technology and digital tools that give the participant convenient options to provide information that’s needed for the trial, to interact with research staff, and to complete study activities.” The use of technology allows participants to complete part of, or in some cases, all the study activities remotely.
If there are parts of the study that cannot be completed remotely, an alternative location can be selected. This may include the participant’s home, workplace or their own doctor’s office. One example is when a mobile phlebotomist is sent to where a patient lives to conduct a blood draw.
“A decentralized clinical trial does not necessarily mean that a participant will never interact in person with a member of the research staff,” adds Adam Samson, Senior Director of Clinical Operations and Customer Success. Decentralized clinical trials can use a combination of approaches to coordinate patient care and study conduct. As in telemedicine, different communication forms are employed including phone calls, video calls and text messaging.
DCTs greatly scale the convenience factor for participants and caregivers. Traditional clinical trials often required long distance travel to the closest research site, hotel stays and time off from work. Removing geographic barriers and eliminating time constraints means that a greater diversity of patients are able to participate. For study data to represent a universal population, diverse participation is essential. DCTs are paving the way to opening clinical trials to populations that historically faced barriers to participation, including minorities and residents of rural communities.
“The term decentralized clinical trials does not refer to just one thing. It might be that everything is done from the participant’s home, or it could be that the participant chooses to go in for certain things. When it comes to the use of technology, it’s important for participants to understand what the details are around the devices and technology, in order to decide whether it’s something they’d be comfortable with,” says Adam.
Patients’ bodies react differently to medications based on characteristics including age, gender, race and ethnicity. By reducing burdens to participating in a clinical trial, DCTs increase access to clinical research to a diverse pool of participants. In turn, the length of time it takes to develop new treatments and therapies can be decreased.
“Participating remotely is just as important as participating in person,” says Arsheen. “Your participation makes a really big difference in moving science forward.”
Learn more about DCTs by accessing the webinar recording here. View CISCRP’s library of webinars and podcasts here.
To search for medical conditions in a specific location, visit our Search Clinical Trials page.
To stay informed about clinical trials, visit our Resources page.

Visit our Library
of Clinical Research Educational Resources.

View Content by Clicking on each Newspaper Title
Value Add Digital News Editions
CISCRP would like to recognize and extend a ‘Thank You’ to Praxis for donating their pro-bono graphic design services to create the full page advertisement. View the advertisement here by clicking on the star.
To participate in this or another upcoming media campaign to continue to build education and awareness about clinical research, please contact Matt Steele at msteele@ciscrp.org.
Written by: Shalome Sine
Project Manager
CISCRP Research Services

The findings of a recent pediatric survey illustrate perceptions and insights on what matters most to patients and their parents. It also offers ways to best support and inform prospective pediatric volunteers and their guardians before, during, and after the clinical research process.
During the month of April 2020, the Center for Information and Study on Clinical Research Participation (CISCRP) conducted an online United States-based survey among 500 parents and their children. The goal of this survey was to gain insight into general perceptions of pediatric trials, preferred channels of communication, key information parents and their children would want about pediatric clinical trials, as well as past or current experiences participating in pediatric clinical trials.
Awareness & Understanding
Parents generally self-report high levels of understanding about clinical research, and generally high willingness to have their child participate in a clinical research study. Awareness, understanding, and willingness to have their child participate was greatest among parents whose children have previously participated in clinical research.
Among children, levels of awareness of clinical research vary by a child’s age, as older children were more likely to have heard of clinical research compared to younger children. Overall, few reported that they understood clinical research “very well.” Though many were not sure whether they would want to participate, 50 percent reported that they would be willing. The top motivation to participate was altruistic, as children wanted to advance science through their participation.
Participation Experiences
During participation, parents reported highly burdensome experiences and high levels of disruption to their daily routine. Top burdens included traveling to the study clinic and having their child complete lab work like blood draws and urine tests. However, the majority of parents said that they received updates or study results once their child finished participation.
Results also indicate that children generally received adequate information about their participation. Ninety-two percent remembered getting information about the clinical trial before they joined, and 85 percent found this information “kind of” or “very easy” to understand. Despite these expectation-set-ting measures, children reported some study requirements as difficult to complete, most notably taking the study medication and undergoing blood draws. However, though children report burdensome study experiences, most indicate that the study exceeded their expectations, and that they would be willing to participate again.
Doctors are Key
A consistent theme throughout the survey findings was the critically important role that healthcare professionals play along the journey toward participation. For example, parents discuss clinical research with their child’s doctors often and cite their child’s doctors as the top way they learn about participation opportunities. Children would also most prefer to learn about clinical research through their doctor. Doctor recommendations were ultimately the top reason that parents decided to have their child participate.
Article from 2020 Clinical Trials Supplement, USA Today. View Supplement Here >

Written by Melissa E. Daley, Communications & Marketing Manager| mdaley@ciscrp.org
“My sister Roseanne and and I love the movie, ‘The Wizard of Oz’. I told Roseanne I felt like I was going to see the Wizard. There was so much that happened before I got to see her, just like a lot happened to Dorothy in the movie, recounts Reverend Donna J. Matlach, about meeting Dr. Sally Wenzel of the University of Pittsburg Medical Center to consult about Donna’s severe eosinophilic asthma. My granddaughter, Phoebe, even said ‘Nana is going to see the wizard!’” Donna’s medical journey has been arduous and at times, terrifying, (Donna has had severe eosinophilic asthma for more than a decade) but her upbeat nature shines through during our conversation about her experience with clinical research participation.
“It can’t be controlled with the typical medications that are used with other types of asthma. It’s another level of asthma – it goes up in levels. Mine is severe, which is the highest level. It took many years to figure out why it couldn’t be controlled,” explains Donna.
I was on mass quantities of corticosteroids taken orally and by inhalation.” The steroids impacted her overall health, including weight gain and brittle bones leading to several fractures.
The severity of her symptoms sapped Donna of her physical strength, but not her inner fortitude. Taking matters decidedly into her own hands, Donna went on a cross-country journey in order to find medical advice and effective treatment. Conducting a lot of research on her own, Donna visited 28 doctors, the majority being pulmonary specialists, in 12 hospitals, nationwide. In a frustrating turn of events, they all provided different diagnoses and advice. To make matters worse, the nebulizer and cortiscosteroid medications Donna was taking were not adequately controlling her illness.
“My asthma was so misdiagnosed that at one point, doctors from a major medical facility told me I should see a psychiatrist. I was on a nebulizer every hour to stop the coughing and wheezing,” says Donna. “I’ve had over 600 allergy tests. I’m not allergic to anything.” Donna continued on her quest for relief from her symptoms. Donna consulted with a physician in Colorado who recommended she meet with Dr. Wenzel.
“Dr. Wenzel is the guru. She founded the University of Pittsburgh Asthma Institute,” says Donna.
During one of her many visits to Pittsburgh with Dr Wenzel, Donna had video assisted thoracic surgery to take biopsies and view her lungs with a camera. “I woke up with a tube in my chest to prevent my lungs from collapsing. The pain was so bad I ended up having a full-blown asthma attack, even with the pain medication pump. I’ve had a lot of surgeries in my life, including two C-Sections, and this was the worst!” says Donna.
Donna has had two 6-hour surgeries on her sinuses in the past several years. Both times, her sinuses were evaluated to be 98% blocked. “I had no taste or smell for 3 years because the sinuses and asthma were impacting each other. Everything is connected,” says Donna. When Donna arrived for the first surgery, she was told her lungs were too weak to undergo the procedure. Dr. Wenzel was concerned she would not survive the anesthesia. When Donna was able to have the first sinus surgery, several months later, Dr. Wenzel advised Donna that the positive results she was experiencing would last about three years.
“Wouldn’t you know it, it was just about 3 years to the month and I needed to have another surgery. Dr. Wenzel was right – that’s why I call her The Wizard,” says Donna. The second sinus surgery removed a bone from the left and right side of Donna’s frontal sinuses.
Dr. Wenzel assisted her with this process, but Donna was told she was not sick enough to participate in the first clinical trial to which she applied. This was perplexing to Donna because, she recounts that “I have been catching pneumonia twice year!”.
Dr. Wenzel located another clinical trial and Donna qualified as a participant. The clinical trial site was in California.
“I flew from my home in Arizona to California, once a month, at my own cost, for three years. I ended up being a poster child for the sponsoring company. I now speak at lectures for them about my experience, in New York City and other places,” says Donna.
The medication she received in the clinical trial in California was not immediately effective. “It took about 6 months to get into your system. At first it was an IV medication, and then it became an injectable,” says Donna. “My asthma is like a firecracker. It will either fizzle out or it will explode.” A couple of years later, that treatment stopped working.
During this time, Donna’s health was also being monitored in her then-home-state of Arizona. “I was at the Mayo Clinic in Scottsdale, waiting for a lung function test, and while I was there, I had a severe asthma attack. It came out of the clear blue sky. I ended up in the ER. God put me in a place where I could be helped and I wasn’t alone. I’ve had three near fatal episodes because of the asthma,” Donna recalls.
After the clinical trial that Donna participated in, Dr. Wenzel prescribed a biologic that had recently come to market. “It took 4 months for it to start working and I took it for a year. But I was still back and forth with ER visits that always turned into a hospital stay, unfortunately,” says Donna.
During her hospital stays, Donna continued to work on her studies towards her Masters of Divinity. Even though she was very ill, Donna says that “God told me… You’re not done.” She subsequently studied several more years and received her Doctorate in Ministry and Master’s in life coaching.
Dr. Wenzel then prescribed a third biologic medication, which was not part of a clinical trial.
“I go to Pittsburgh twice a year to see Dr. Wenzel and we’ve become close friends. I love her. My heart told me, when I met her, that this was going to be the best doctor I could possibly see,” says Donna, smiling.
Donna’s family was supportive of her decision to join a clinical trial. She looked for patient advocacy organizations for severe asthma, and there were none established at that time.
Donna has experienced, first-hand, the serious impacts of severe asthma. “It’s not just physical. It effects your emotional well-being. It effects your family, your day-to-day life, your finances. No one ever asked me about those things, in doctor’s appointments – not until I met Dr. Wenzel,” says Donna.
“Why would you not? You could have side effects, but for me, how could it be any worse, since I was having near fatal episodes? You have to keep searching. Clinical trials can be the answer. Why would you not want to try it? This is why I am a patient advocate. I love sharing information about clinical trials with people. That’s why I went into the ministry. I know God has a purpose for my life to reach out to people with similar physical issues as a friend, minister, and counselor. ”
To search for medical conditions in a specific location, visit our Search Clinical Trials page.
To stay informed about clinical trials, visit our Resources page.
Written by: Scott Finger | sfinger@ciscrp.org

Dear readers,
If you have been following CISCRP and our newsletter, you know about some of the exciting and innovative changes we have made over the last year and a half. While we understand it can be tiring to hear so much about the pandemic and the “new normal,” we can’t overstate how important it is to continually address disparities in health care and clinical research. In this issue, we cover some of the changes we have been making and what you can expect from us in the coming months.
One of CISCRP’s biggest initiatives has been to address the inequity of participation in clinical trials. In other words, we want to turn underrepresented communities into represented communities. Our Health Literacy team is collaborating with members of these communities to learn how we and clinical trial professionals can bridge the gap. We will add this knowledge to our library of educational brochures, so stay tuned for the finalized publications. Also in this issue, we discuss how our AWARE for All live educational series focuses on diversity and inclusion. Our next event is happening October 21, and our final AWARE event of the year will be held on November 18.
Our efforts would not be possible without our Research Services team having important conversations with the community. The results of our Perceptions & Insights Study, conducted every two years, will be available this fall! Read here for a sneak peek of some of the key findings, including responses from members of ethnically and racially underrepresented communities.
In our Supporter Spotlight article, Luther T. Clark, MD, Deputy Chief Patient Officer of Merck, explains some of the other issues surrounding healthcare disparity. These issues include the pandemic, social and economic factors, and certain groups’ lack of access to technology (known as the “digital divide”). With in-person interactions becoming rarer, it is important now more than ever to help communities without the proper resources.
CISCRP is also taking steps to make research results more accessible. The results of clinical trials and other scientific studies are incredibly complex, and there is a large demand for plain language information. In response, we have partnered with sponsors and other experts to create “plain language summaries of publications” (PLSPs), which turn hard-to-understand articles into easy-to-understand summaries. This new offering expands our plain language portfolio to include not only trial results summaries, but all types of scientific and medical articles.
It takes a community to make change, and that is absolutely true when it comes to clinical research. In this issue, we highlight the efforts and the experience of CISCRP’s own Phyllis Kaplan in our ongoing Medical Hero Spotlight series. Read here to learn more about Phyllis’ journey from patient and advocate to clinical research participant to Senior Manager of Events & Community Engagement at CISCRP.
While the clinical research community has become more aware of the disparity in representation, clinical trials are still not as diverse as they should be. We still have much work to do to address the knowledge gaps that exist within the general public. Whether you are a health professional or member of the community trying to do your part, we encourage you to learn as much as you can about clinical trials and the important issues we need to address. As a team, we can make a difference to ensure that all voices are heard, and that research accounts for people of all backgrounds.
Take care, and stay safe,
Scott Finger
Editor, Health Literacy


Written by: Melissa E. Daley, Communications & Marketing Manager, CISCRP
Phyllis has a vague recollection of waking up in a hospital with tubes attached to her body, and a distinct memory of saying, “Take the tubes out!” At the age of two, she was diagnosed with type 1 diabetes, an autoimmune disease, typically diagnosed in childhood, but can manifest at any age. Diabetes has led Phyllis on a path from patient to advocate to clinical research participant.
“I have been an advocate since I was 12 years old. It started in junior high school, in a gym class when the teacher made me take off my medical alert bracelet, due to a ‘no jewelry in gym class’ rule,” says Phyllis. When she went to retrieve the medical bracelet from the gym locker after class, she discovered it had been stolen. This incident spurred Phyllis to write a letter to the town superintendent of schools, demanding its replacement and a change in the rule to allow medical-related items to be worn. By the time the letter had been delivered, the bracelet had been anonymously returned to the school’s lost & found box. Phyllis was allowed to wear the bracelet moving forward.
Type 1 diabetes develops quickly. The body’s immune system attacks and destroys beta cells in the pancreas that create insulin. The body cannot produce insulin without these beta cells. Insulin is a peptide hormone that helps your body metabolize fats, proteins and carbohydrates through glucose (a type of sugar) that is released into the bloodstream when you eat food. The glucose is then absorbed from the blood in the liver, fat and skeletal muscle cells. Type 2 diabetes develops more slowly, over time. The body produces insulin, but cannot use it effectively.
Decisions about how much medication to take are based on many variables including food, exercise, change in weather, change in personal schedule, and stress.
“That’s why education is so important,” says Phyllis. “If I am going to exercise, I have to plan ahead, at least a couple of hours before, as exercise impacts blood sugar. There are so many hidden things to know about diabetes that impact your decisions.”
“As a longtime advocate, I felt that participating in a clinical trial was the ultimate form of advocacy,” Phyllis explains.
“The trials were very different from each other,” says Phyllis. “Two of the three were very easy. One involved two full days in clinic, and that was really hard, with nine hours of ongoing blood tests. Those were physically difficult days, but worth it. The other two clinical trials were less invasive.”
When considering the two-day, in-clinic trial, Phyllis and her husband reviewed the protocol together. “I wouldn’t participate without consulting him,” says Phyllis. He accompanied her to the two in-clinic days, to be with her during the nine hours of ongoing tests and to lend additional support.
When asked if she faced any concerns from family or friends about her clinical research participation, Phyllis says, “No, quite the opposite. People were really interested in the ‘why’ of what I was doing and what the outcomes were.” Phyllis didn’t seek any advice from patient advocacy organizations, because of her own experience as an advocate. She is a brand ambassador with Medtronic Diabetes to share her experience with their medical device, and also volunteers with JDRF (Juvenile Diabetes Research Foundation) and ADA (American Diabetes Association).
Read the protocol and informed consent, which can be confusing. Use a highlighter to mark items in the protocol or use Post-its to make notes. Keep asking questions throughout the course of the study. At times the research staff may not always be patient-centric, and if you’re not getting the answers to your questions, ask to speak with someone else on the study team. Be your own best advocate and keep pushing. Researchers are not always prepared to answer patients’ questions. If something doesn’t sit well with you, voice it.”
Her experience as a clinical trial participant has strengthened Phyllis’ commitment in sharing information about the importance of clinical trials to everyone. Phyllis is adamant and passionate about participating in clinical research again if the opportunity presents itself, reiterating,
To search for medical conditions in a specific location, visit our Search Clinical Trials page.
To stay informed about clinical trials, visit our Resources page.

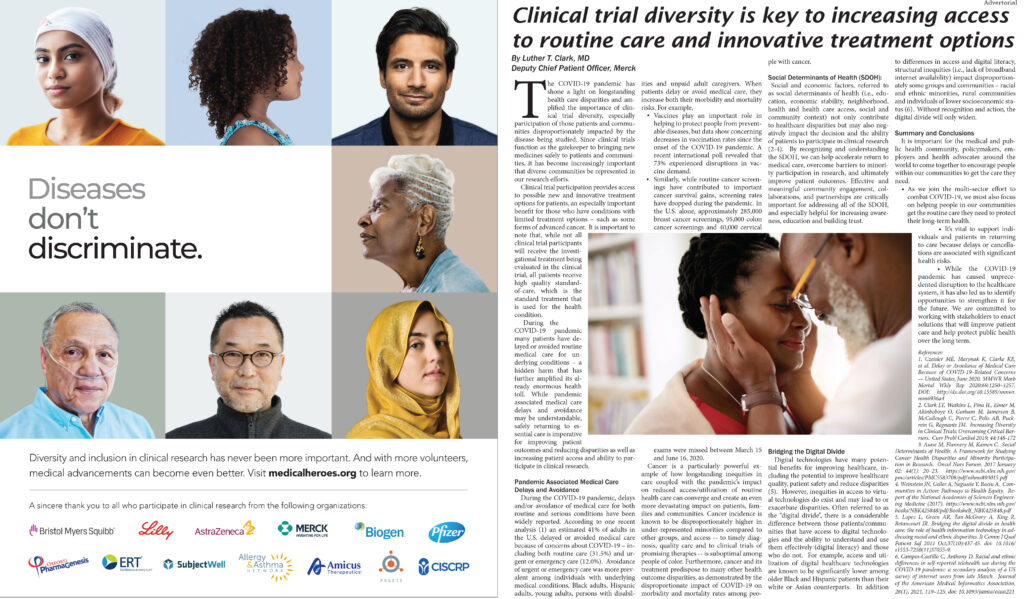
By: Luther T. Clark, MD, Deputy Chief Patient Officer, Merck
The COVID-19 pandemic has shone a light on longstanding health care disparities and amplified the importance of clinical trial diversity, especially participation of those patients and communities disproportionately impacted by the disease being studied. Since clinical trials function as the gatekeeper to bringing new medicines safely to patients and communities, it has become increasingly important that diverse communities be represented in our research efforts.
Clinical trial participation provides access to possible new and innovative treatment options for patients, an especially important benefit for those who have conditions with limited treatment options – such as some forms of advanced cancer. It is important to note that, while not all clinical trial participants will receive the investigational treatment being evaluated in the clinical trial, all patients receive high quality standard-of-care, which is the standard treatment that is used for the health condition.
During the COVID-19 pandemic many patients have delayed or avoided routine medical care for underlying conditions – a hidden harm that has further amplified its already enormous health toll. While pandemic associated medical care delays and avoidance may be understandable, safely returning to essential care is imperative for improving patient outcomes and reducing disparities as well as increasing patient access and ability to participate in clinical research.
Pandemic Associated Medical Care Delays and Avoidance
During the COVID-19 pandemic, delays and/or avoidance of medical care for both routine and serious conditions have been widely reported. According to one recent analysis (1) an estimated 41% of adults in the U.S. delayed or avoided medical care because of concerns about COVID-19 – including both routine care (31.5%) and urgent or emergency care (12.0%). Avoidance of urgent or emergency care was more prevalent among individuals with underlying medical conditions, Black adults, Hispanic adults, young adults, persons with disabilities and unpaid adult caregivers. When patients delay or avoid medical care, they increase both their morbidity and mortality risks. For example,
Cancer is a particularly powerful example of how longstanding inequities in care coupled with the pandemic’s impact on reduced access/utilization of routine health care can converge and create an even more devastating impact on patients, families and communities. Cancer incidence is known to be disproportionately higher in under-represented minorities compared to other groups, and access — to timely diagnosis, quality care and to clinical trials of promising therapies — is suboptimal among people of color. Furthermore, cancer and its treatment predispose to many other health outcome disparities, as demonstrated by the disproportionate impact of COVID-19 on morbidity and mortality rates among people with cancer.
Social Determinants of Health (SDOH)
Social and economic factors, referred to as social determinants of health (i.e., education, economic stability, neighborhood, health and health care access, social and community context) not only contribute to healthcare disparities but may also negatively impact the decision and the ability of patients to participate in clinical research (2-4). By recognizing and understanding the SDOH, we can help accelerate return to medical care, overcome barriers to minority participation in research, and ultimately improve patient outcomes. Effective and meaningful community engagement, collaborations, and partnerships are critically important for addressing all of the SDOH, and especially helpful for increasing awareness, education and building trust.
Bridging the Digital Divide
Digital technologies have many potential benefits for improving healthcare, including the potential to improve healthcare quality, patient safety and reduce disparities (5). However, inequities in access to virtual technologies do exist and may lead to or exacerbate disparities. Often referred to as the “digital divide”, there is a considerable difference between those patients/communities that have access to digital technologies and the ability to understand and use them effectively (digital literacy) and those who do not. For example, access and utilization of digital health care technologies are known to be significantly lower among older Black and Hispanic patients than their white or Asian counterparts. In addition to differences in access and digital literacy, structural inequities (i.e., lack of broadband internet availability) impact disproportionately some groups and communities – racial and ethnic minorities, rural communities and individuals of lower socioeconomic status (6). Without recognition and action, the digital divide will only widen.
Summary and Conclusions
It is important for the medical and public health community, policymakers, employers and health advocates around the world to come together to encourage people within our communities to get the care they need.
This article was also featured in our Patient Diversity Campaign. See Campaign Here.
References:

By: Jessica Cronin | jcronin@ciscrp.org
CISCRP is excited to announce that the full results of the 2021 global Perceptions & Insights Study will be available this fall! This latest study contains insights from nearly 12,000 individuals around the world on various aspects of clinical research — including the impact of the COVID-19 pandemic on awareness and perceptions, as well as thoughts on and experiences with clinical trials that require fewer visits (decentralized trials). These results uncover significant new findings on patient engagement preferences and ways to increase access, particularly among underrepresented communities.
Our 2021 study captured the experiences of over 5,500 trial participants across diverse therapeutic areas, which was nearly 2,000 more participants than in previous years!
Key findings from the 2021 Perceptions & Insights Study include:
Since 2013, CISCRP has conducted the Perceptions & Insights Study every other year to monitor trends and identify opportunities to better inform and engage the public and patients as partners in the clinical research enterprise.
To review these findings and more from the 2021 Perceptions & Insights Study, CISCRP will be hosting a webinar in October, as well as posting reports on the CISCRP website. If you would like to register for the webinar – please go to here.

Written by: Joan Chambers | jchambers@ciscrp.org
CISCRP and Oxford PharmaGenesis collaborated with Daiichi Sankyo, AstraZeneca, and Dr. Shanu Modi of the Memorial Sloan Kettering Cancer Center in New York to write a plain language summary publication (PLSP) of the results of the DESTINY-Breast01 clinical trial.
The demand from the public, patient, and health care communities for plain language information on results of clinical trials is extremely high. For more than ten years, CISCRP has been translating scientific clinical trial results information into plain, easy-to-understand language for patients and the public around the world to be communicated in print and digital formats.
This PLSP provides important information about HER2-positive breast cancer to patients, their family members or caregivers, and patient advocates. In a simple format, the PLSP highlights and addresses: what HER2 positive breast cancer is, why the clinical trial was conducted, the most common adverse events, and the overall trial results.
Over 253 women aged 18 and older participated in the trial. This PLSP answers the main questions researchers had in the DESTINY-Breast01 trial:
The PLSP team worked to ensure the PLSP was easy to read by adding creative visuals, tables, and answers to key questions about the DESTINY-Breast01 clinical trial. The PLSP was reviewed by an editorial panel of patients, patient advocates, members of the public, and healthcare professionals to evaluate and confirm that a “patient-first” approach was taken. The panel reviewed the writing, design, and layout to help patients, family members, and caregivers understand the trial results.
Read the full published PLSP on Future Oncology here.
CISCRP collaborates with industry organizations to create documents from scientific manuscripts that are accessible for patients, patient advocacy groups, and the public. Visit Health Communication Services for more information.
I graduated with my master’s in medical anthropology from Boston University School of Medicine in 2016. Prior to starting at CISCRP, I worked on research studies focused on patient experiences with health care. Most recently, I worked on several projects related to substance use and people living with HIV. I am incredibly passionate about working with vulnerable populations and increasing access to care for patients through research. As Project Manager in Research Services, I am excited to connect with new patient groups and make research more approachable for vulnerable populations.


Dominantly Inherited Alzheimer’s Disease Brochure
Expanded Registry Flyer (English)
Enfermedad de Alzheimer de herencia dominante
Expanded Registry Flyer (Spanish)
Forgetting the Little Things
Concerned About Memory Loss?




Click on the resources listed below to view the full versions of LCI’s materials.


Krysal Doucet has worked in Research as a CRC for 11 years and as an Associate Site Director for 2 years. She started her path in the health care industry by becoming a C-MA. After completing the Medical Assisting course, she was introduced to a great opportunity working as a Clinical Research Coordinator with Benchmark Research.

Missy Hansen MSN, APRN, CPNP, CPHON, joined ICON in 2019 as a pediatric strategy liaison. She has 25+ years of experience as a pediatric nurse practitioner, including 17+ years in pediatric hematology/oncology at Children’s Minnesota, the largest hematology/oncology service line in the region, providing care for infants through young adults diagnosed with hematologic and/or oncology conditions. Ms. Hansen gained expertise working in inpatient, outpatient, and urgent care type settings. Ms. Hansen has in-depth experience working with the Children’s Oncology Group—the largest consortium with the most open pediatric studies around the world. She also has experience working with other consortia that conduct trials for pediatric to young adult patients.
Lori Ranney DNP, APRN, CPNP, CPHON has worked in pediatric oncology for 20 years and has been a PNP at Children’s Minnesota for over 13 years. She has a special interest in leukemia/lymphoma, patient/family education, AYA population, and oncofertility. She is a member of the Children’s Oncology Group and has actively enrolled patients in clinical trials for over 15 years.
Mark has over 20 years of experience in the pharmaceutical and biotech industries and currently leads ICON’s global pediatric center of excellence. Having earned his medical degree and master’s degree in clinical nutrition from the Chicago Medical School, Dr. Sorrentino completed both a residency in pediatrics and a fellowship in pediatric critical care at Children’s National Medical Center (CNMC) in Washington, DC. Currently, Dr. Sorrentino holds an appointment as an assistant clinical professor at the George Washington University School of Medicine. Prior to joining the industry, Dr. Sorrentino was an attending physician in the CNMC pediatric intensive care unit for 8 years and participated in numerous industry-sponsored critical care trials. He holds active medical licenses in California and Maryland.
Based in Minnesota, Dr. Perkins has 21 years of experience in clinical research across Phases I–III with a focus on hematologic malignancies. Before joining ICON in 2018, she was in clinical practice for 15 years specializing in leukemias, lymphomas, and long-term complications of cancer therapy. Dr. Perkins has supported multiple oncology/hematology trials across indications and phases. She is board certified in pediatrics and pediatric hematology and oncology and holds a master’s degree in clinical research.

Christian oversees the development of new strategic partnerships, products and services to help shorten the diagnostic odyssey, improved access to research and help expand the number of treatments available for all rare disease patients and caregivers.

Dr. Dastgir specializes in pediatric neurology and is the director of the pediatric neuromuscular medicine program at Goryeb Children’s Hospital in Morristown, NJ. Her current practice is primarily composed of patients with rare disorders.
Dr. Dastgir also has experience in being an investigator for clinical trials involving such rare conditions as spinal muscular atrophy, duchenne muscular dystrophy, and infantile neuroaxonal dystrophy.

Generally, chronic health conditions greatly impact the lives of those within a household, not just the patient, but also the caregiver(s) and other members of the family; because of this, Mel has made it her mission to rise above the health obstacles within her own family and help others gain the knowledge and confidence to do the same. Having a chronic condition does not define a person, while it may affect the quality of one’s life, it does not need to become an unsurpassable obstacle preventing one from exploring their dreams and living life to the fullest.
Mel loves speaking publicly and jumps at every opportunity to do so, she has spoken at schools, rallies, congregations and even at the California State Capitol; no audience is too big or too small. She is passionate about helping people gain confidence in themselves, to learn self-advocacy, to find their voice and gain the inner strength to effectively be heard, and to live life to its absolute fullest potential.

Jenn McNary is a trusted voice in the rare disease community, as a mother, public speaker and fierce advocate. Her work in the rare disease space as a thought leader earned her the Ryan’s Quest Ryan’s Hero award in 2013, a nomination for the Global Genes Champion of Hope award in 2014, and the prestigious 2017 Meyer- Whalley instrument of change award. Formerly as the director of outreach and advocacy at a Massachusetts based non-profit foundation, she was responsible for the organization of the largest FDA advisory committee hearing in history, with over 1000 duchenne advocates, families, clinicians and researchers in attendance.
Jenn has unique experience in the drug development field, as a parent of children enrolled in the clinical trials, an advocate engaging with the regulators and as a consultant helping to develop programing for patients. Currently, Jenn is consulting in the biotechnology space with an expertise in caregiver/patient engagement, including bringing the patient voice to drug development and solving barriers to access.
Her other activities include serving as the Founder of One Rare, a non-profit formed to meet the needs of young adults with rare and chronic conditions and raising her four children in Massachusetts.

Mr. Schliebner is a clinical development executive with a 25-year background focused on rare diseases, innovation, and patient-focused approaches to drug development. He is passionate about reducing the burden of clinical trial participation and leveraging novel approaches and technologies to bring new therapies to patients faster. Mr. Schliebner also serves as the Co-Chair of Global Genes’ Corporate Alliance, serves on the Board of Directors for Uplifting Athletes, and supports several rare disease panels and committees. He holds a Master’s Degree in Public Health (MPH) from the University of Utah School of Medicine, and completed a Graduate Research Fellowship at The National Institutes of Health.

Cristol Barrett O’Loughlin is a seasoned executive and storyteller. As Founder and CEO of Angel Aid Cares, Cristol is fiercely passionate about providing social, emotional, physical and financial relief to mothers of children with rare disease. A former UCLA instructor, she co-founded the advertising firm, The Craftsman Agency, and is humbled to advise global brands; NBA, Disney, Fox, Cisco Systems and Google. During her tenure at IBM Life Sciences, she helped accelerate advancements in cheminformatics and biotechnology. She presented a TEDx talk “Caring for the Caregivers: 3 Tools for Self-Care”.

Rosamund Round leads Parexel’s Patient Innovation Center, focused on improving research access and experiences for patients and caregivers. This includes leadership of the decentralized clinical trials service, activities to improve diversity in clinical research, and creation of other tools and services that reduce practical, financial and geographical barriers to participation.
She has 17 years of leadership experience in patient engagement and innovation roles, and regularly presents and authors articles on the topic.

Liam Paschall is a transgender man who has found immense courage, power, and pride in accepting the truth of who he is. His pronouns are he and him.
He is an entrepreneur, public speaker, and facilitator, with a lifelong goal of changing hearts and minds – one person at a time. He is a passionate servant to the LGBTQIA+ community with the ability to motivate and inspire others to live out loud.
Having started his female to male transition at the beginning of last year, Liam knows first-hand how critical and life-altering inclusive healthcare and clinical trials can be to members of the LGBTQIA+ community.

Dr. Sebastian Barr is a licensed psychologist currently based in Western Massachusetts. He received his PhD in Counseling Psychology and completed advanced training in health service psychology and psychotherapy research at Cambridge Health Alliance under the auspices of Harvard Medical School. His scholarship centers on the experiences, mental health, and mental healthcare needs of members of the trans community, with a particular recent focus on the impacts of bias and non-affirmation. His research has been recognized nationally and internationally and published and cited across multiple journals and textbooks. Additionally, he specializes in helping institutions and healthcare providers adopt affirming, inclusive, and evidence-based practices in both clinical work and research with members of the trans community. He is a proud transgender man and incorporates personal lived and community experience into his work.
For over a decade, Adam has conducted clinical trials across multiple therapeutic areas as a research coordinator, monitor, project manager, and director at various types of organizations—investigational sites, CROs, academia, pharma, and tech. He received a master’s in clinical research from The George Washington University. In June 2020, he joined as Director of Clinical Operations at Curebase, a provider of software and services purpose-built for decentralized clinical trials (DCTs), where he is responsible for oversight of DCT services.

Arsheen Ali is a Project Manager and has served in this role with Curebase for over two years. In this capacity, she manages multiple decentralized clinical trials. Her background includes a variety of healthcare and research experience. She received her bachelor’s in integrative biology from UC Berkeley. Arsheen’s main interests are public health (population and community health focus), increasing healthcare quality and access (especially for minority/marginalized populations), and maximizing the efficiency of research.

Myra Lane is Lead Virtual Research Coordinator at Curebase with over three years of clinical research experience in the decentralized clinical trial space interacting directly with patients. She has worked in various therapeutic areas including neurology, dermatology, and oncology. She is passionate about the impact that the digital therapeutics approach has on addressing unmet patient needs by providing universal access to clinical research and accelerating the development of treatments.

Ken Getz is the founder of CISCRP and chairs the board of directors. He is also a professor and the Director of the Center for the Study of Drug Development, Tufts University School of Medicine where he conducts grant-funded studies on pharmaceutical R&D management and execution; protocol design optimization; contract service provider and investigative site management; e-clinical technology and data usage; and patient engagement. Ken is the founder of CenterWatch, a leading publisher in the clinical trials industry and one of several companies that he has created and sold. A well-known speaker at conferences, symposia, universities and corporations, Ken has published numerous articles and chapters in peer-review journals, books, and in the trade press. He is the author of two nationally recognized books for patients and their advocates including The Gift of Participation, and the recipient of several awards for innovation and scholarship. Ken has held a number of board appointments in the private and public sectors, including serving on Otsuka’s Patient Assistance Foundation, the Institute of Medicine’s Clinical Research Roundtable, the DIA Foundation, the Consortium to Examine Clinical Research Ethics, and the Clinical Trials Transformation Initiative.

At CISCRP, I manage the design, implementation, analysis and reporting of a variety of CISCRP research studies. I have more than 15 years of experience conducting primary and secondary research studies in the healthcare, life sciences and consumer goods industries. Prior to CISCRP, I worked at Colgate-Palmolive as a research manager. I hold an MBA from the Graduate School of Management at Boston University and a Bachelor of Science degree from Bryant University. I am passionate about helping others, and CISCRP offers ample opportunities in that regard. People often comment that I am a nice and genuine person. And I think those characteristics help me connect to the patients I interact with regularly through my work. I especially enjoy being involved in bringing patients and clinical operation teams together through the CISCRP Patient Advisory Boards; speaking with each other about ways to make clinical trials a better experience overall is very rewarding for me.

As a Peace Corps Volunteer, I served as an English Literacy Facilitator in the Kingdom of Tonga. There, I gained invaluable experience working alongside my community and counterparts through projects such as student-centered learning initiatives within the classroom, grant writing for better access to technology, establishing a school library, as well as promoting girl’s empowerment and opportunities for fitness and healthy living. Throughout my service, my favorite experiences were always connecting with individuals in the community – exchanging stories, cultures, traditions, and laughter. Additionally, I am a graduate of Connecticut College where I earned a B.A. in Psychology and an Elementary Education certification. I am excited to have the opportunity to apply my love of education, psychology, and research through my work at CISCRP. As a Project Manager, I enjoy working with a variety of individuals from diverse backgrounds and experiences to help amplify the patient voice within clinical research trials.

I graduated with a B.A. in Sociology from Skidmore College in May 2020. At Skidmore, I worked on multiple research projects including a journal article I co-authored with a professor focusing on Tor and the Dark Web, as well as my Senior Thesis, which examines the relationships between mental health and access to natural environments. Through my research projects, as well as my education in Sociology, I learned the importance of using research to improve access to crucial resources and institutions that help communities grow and thrive. I also had the opportunity to intern for Habitat for Humanity, which strengthened my interest in working for a non-profit organization that aims to overcome barriers in the way of essential resources such as housing or healthcare information. I am excited to use my research experience and my love for working with people to help improve the clinical research process, and highlight the patient experience as central to the development of clinical trials.

Kim Harper, began her clinical research experience as a Clinical Research Coordinator back in 2007. Over the next 7 years she worked as a CRC gaining experience working for an arthritis clinic and a research center. In 2014, Ms. Harper was brought on by Benchmark Research, a leading clinical research firm as a CCRC. She quickly worked her way through the ranks to Assistant Site Director and in 2020 Kim became promoted to Site Director.
During her 14 years in the field, Kim has been a significant contributor to the studies she has worked on which include Phase 1-4 treatment, preventative and diagnostic trials on pediatric, adult, and elderly subjects. Kim has diverse experience in vaccine, drug, and device trials as examples therapeutic areas she has worked on include ebola, anthrax, COVID-19, diabetes, influenza, meningococcal, antipsychotics, depression, alzheimer’s disease, osteoarthritis, and more. During the COVID-19 pandemic, Kim thrived in the high pressure environment and led her North Shore New Orleans research site to successfully conduct 2 coronavirus studies including a high profile vaccine. Kim is known amongst her peers for her proven ability to reach across personal and professional barriers to expedite effective health care.

Stephanie is a patient advocate at The Young Face of Arthritis.

As a rare disease patient living with primary lymphedema (LE) for over three decades, Britta remains determined to challenge her limits rather than to let LE limit her challenges. Despite wearing compression garments 24 hours a day, she has skied Mount Tremblant, completed the 10k Chesapeake Bay Bridge Run, and climbed the Great Wall of China. Britta pays it forward by sharing “advice, comfort, and positive thinking” on her award-winning blog, lymphedemadiary.com. As Senior Director of Communications and Marketing for the EveryLife Foundation for Rare Diseases, Britta initiates strategies that inspire patients and caregivers to engage in advocacy and make their voices heard. Britta lives in Arlington, Virginia with her husband and two very spoiled cats.

Ryan Colburn is a guy with 2(+) typos on his GAA gene on chromosome 17. He has a professional background in engineering and operations management; spending portions of his career working on race cars, airplanes, and rockets. Diagnosed with Pompe disease in 2015, he has spent the time since learning about rare disease topics including research, advocacy, and development of treatments to better understand how to participate in the rare disease ecosystem. He is passionate about patient empowerment and engagement; actively developing relationships with other patients, advocacy groups, researchers, and pharmaceutical companies. He is driven to improve the health of the rare disease ecosystem by shifting the view from patients as “subjects” to one of participants, collaborators and partners who help find the most effective ways to tackle the challenges of rare disease and break down barriers to the acceleration of progress. Ryan has participated in nine clinical studies since he was diagnosed, and has shared his perspectives with industry and advocacy organizations to improve the patient experience within the clinical research space.

Dr. Kim Stephens is the president of Project Alive, a nonprofit organization dedicated to research and advocacy for Hunter syndrome. Project Alive that is a powerful voice for children and adults with Hunter syndrome and brings together families and advocates with researchers, industry, and regulators. Having a son with Hunter syndrome herself, this is also a personal mission for Kim. Her son Cole has been participating in a clinical trial for the past 6+ years. Having gone through the ups and downs of clinical trial life, Kim is a strong advocate for creating better outcome measures, integrating the patient voice in trial design, and considering the entire cycle of the clinical trial – from the patient’s doorstep to the clinic and back home again. She frequently speaks as a rare disease advocate at conferences and events and serves as a mentor and resource for newly-diagnosed families.
Kim is also the founder of Inclusive Thinking – a consulting company dedicated to increasing diversity and inclusion through research, education, and strategic planning. Before founding Inclusive Thinking, she had a twenty-year career with IBM, most recently as the Global Diversity & Inclusion Communication and Education Lead. She has spoken at conferences around the world and conducted workshops on unconscious bias, cultural awareness, women’s leadership, accessibility, and other topics.
Kim earned her doctorate in Business from Georgia State University and focused her dissertation on implicit bias and the role of transformational conversation and social identity on behavioral change.

Marc Yale was diagnosed in 2007 with Cicatricial Pemphigoid, a rare autoimmune blistering skin disease. Like others with a rare disease, he experienced delays in diagnosis and difficulty finding a knowledgeable physician. Eventually, Marc lost the vision in his left eye from the disease. This inspired him to help others with the disease. In 2008, he joined the International Pemphigus and Pemphigoid Foundation (IPPF) as a Peer Health Coach. He worked with people to improve their quality of life and encouraged them to become self-advocates. In 2009, he helped develop the Pemphigus and Pemphigoid Comprehensive Disease Profile giving experts insight into the patient perspective. In 2016, Marc became the Executive Director of the IPPF. He has recently become the Advocacy & Research Coordinator of the IPPF so that he can focus on research and advocate for all of those affected by pemphigus and pemphigoid. He is a member of the American Academy of Dermatology Drug Transparency Task Force, sits on the Executive Board of Directors for The International Alliance for Dermatological Patient Organizations as their Treasurer, serves on the Board of Directors of Haystack Project, and is a committee advisor for Rare Disease Legislative Advocates. Marc recently joined Rare Disease International in the establishment of the WHO Collaborative Global Network for Rare Diseases Panel of Experts to ensure a lasting impact on the lives of people living with a rare disease around the globe.
Marc currently resides in Ventura, California with his wife of 31 years.

Mike Wenger is Global head of Patient Engagement at Informa Pharma Intelligence. As both a patient and software developer, Mike is passionate about patient access to clinical trials. He is spearheading Citeline Connect, the only end-to-end platform for clinical trial education, recruitment and enrollment, enabling sponsors to accelerate study startup and boost engagement. Mike was named one of the 2020 PM360 ELITE 100 in the Patient Advocates category and a 2020 Force for Change Illuminator. He also was a finalist in the Patient Advocate of the Year category in the 2020 Medigy HITMC Awards.

Wes Michael founded Rare Patient Voice in 2013 to give patients and caregivers with rare diseases the opportunity to voice their opinions in research studies. Rare Patient Voice has now conducted thousands of studies and rewarded patients and caregivers with over $8 million for their participation. Many have been recruited in person by Wes and his team at patient events like fund-raising walks and patient conferences, and through a referral program with patient advocacy and support groups. Rare Patient Voice now covers non-rare as well as rare diseases and conditions and has expanded from the United States to Canada, the United Kingdom, France, Germany, Italy, Spain, Australia, and New Zealand.
Before launching Rare Patient Voice, Wes worked for healthcare market research firm Kantar Health. He previously was a brand manager and market research manager at McCormick (the spice company) and General Mills (working on Wheaties, Total and Kix cereals). He has a BA from the University of Pennsylvania (with a year at Edinburgh University) and an MBA from the University of Chicago. Wes was recently inducted into the DTC National Hall of Fame, honoring individuals who have demonstrated extraordinary achievement in the advancement of direct-to-consumer marketing.

Steve Jones, is President of EU-IPFF, the European Idiopathic Pulmonary Fibrosis and Related Disorders Federation and part of the Citeline Connect referral collective. EU-IPFF is dedicated to making clinical trials work better for patients in partnership with pharma and regulators in UK and Europe. Steve also is chair of trustees of the UK patient organization Action for Pulmonary Fibrosis and a council member for the European Lung Foundation. He also sits on the steering committees of four major non-pharma clinical trials funded by the UK’s National Institute of Health Research. Steve himself is a pulmonary fibrosis patient and had a lung transplant five years ago.

Ashley Smock is a woman living with ovarian cancer. She took part in the Rare Patient Voice/Informa survey on patients and clinical trial participation in 2021.

Amy brings a comprehensive understanding of drug discovery and drug development from the research laboratory to patients’ bedside from 20+ years of experience in academic institutions, biotech companies, and CROs. Originally trained as a molecular biologist, she transitioned into drug development and came up through clinical operations before joining the Center for Rare Diseases in 2017. She has contributed to discovery and development of treatments for many rare disease patient communities, from rare cancers to rare neurodegenerative disorders, including development of a gene therapy treatment now commercially available to rare disease patients.
Amy leads the Gene Therapy Think Tank and is a Subject Matter Expert in the Center for Immuno-Oncology, Cellular, and Gene Therapy. She provides full life cycle support for gene therapy programs outside of oncology, from study design through study close out. This includes close collaboration with sponsor teams, study physicians, clinical operations throughout the program, as well as supporting integration of patient partnership into clinical operations. She is passionate about enhancing the efficiency of clinical trials through cooperative productivity and patient-centered design – key elements of “Market Aware” clinical development protocols, and a proven pathway to commercial success.

Laura Iliescu, MSc, has 20 years of experience in development and commercialization of therapies, and patient-centered healthcare services. She has held strategic development roles in rare and complex conditions in leading pharmaceutical, biotechnology, CRO and clinical homecare organizations. Her varied experience comprises strategic development throughout every phase of the product lifecycle from pre-clinical to beyond patent expiry in North America and Europe. She has deep experience in rare metabolic, rare neuromuscular an rare respiratory indications among others.
Her background in human factors engineering and user-centered service design methods informs her passion for patient-centered development and for evolving the clinical development paradigm around patients as key stakeholders.
In her current role within ICON’s Center for Rare Diseases, Laura advises product development companies on patient-centered clinical strategy to optimize both study efficiency and the experience of rare disease patients and caregivers. She leads the Center’s Patient Advocacy Strategy team, who support collaboration between companies and rare disease Patient Advocacy Organizations through study design and conduct.
Laura grew up in Toronto, Canada, after which her career (and love of travel) have taken her to more than 40 countries in North America, Europe and Asia. She currently lives in Toronto, Canada with her partner and has both family and friends who are affected by rare conditions. Laura holds a Masters of Human Factors and Ergonomics from the University of Nottingham.

Kelli Wright is the Senior Manager of Patient Advocacy for Harmony Biosciences working to keep Patients at the Heart of everything we do at Harmony. It’s critical to include the patient voice in drug development efforts and Kelli is honored work with patient communities, people living with rare neurological diseases, caregivers, and patient advocacy organizations to share their lived experiences across functions at Harmony.
With a 15+ year non-profit career, Kelli has a deep understanding of the patient needs and experiences. Most recently Kelli was the National Director of Strategic Initiatives for CureSearch for Children’s Cancer, driving the strategic program of CureSearch by staying in tune with the barriers in drug development. Kelli learned from innovators in the industry, academic and regulatory space, as well as patients and disease-foundations, to address obstacles and develop action plans to close the communication gaps and reduce duplication of efforts.

Kendall is a driven health advocacy professional with strong community outreach, patient association, health care provider, rare disease and chronic illness expertise. She specializes in patient advocacy throughout rare disease clinical drug development. She currently serves as the Patient Advocacy Lead, Early Development , at Spark Therapeutics. In this role she supports Sparks preclinical and early clinical development programs. Previously, Kendall served as a Patient Advocacy Strategy Lead at PRA Health Sciences and as the Director of Strategic Alliances at Global Genes, a leading rare disease patient advocacy organization. She has held key roles in patient advocacy and patient education in both the nonprofit and biopharmaceutical industries. Kendall’s passion is to improve the health outcomes of individuals living with rare diseases while integrating advocacy strategy into clinical drug development. Kendall specializes in cultivating partnerships with patient advocacy organizations, identifying and partnering with Key Opinion and Community Leaders, identifying business needs, developing customized programs to achieve key outcomes and balancing a global focus with national, regional and local patient centric partnerships. Kendall works with leaders in the rare disease nonprofit community & biotechnology space to advance progress in rare disease drug development. Kendall also serves on the board of directors of Team Telomere and as a strategic advisor to the Rare and Undiagnosed Network. She holds a Master’s Degree of Public Health from Michigan State University as well as a Bachelor’s of Science in Psychology from Loyola University, Chicago. Kendall currently lives in Pittsburgh, PA with her husband, son and dachshund.

Sarah Nechama Frisch is a woman living with narcolepsy with cataplexy. She took part in the Rare Patient Voice/Informa survey on patients and clinical trial participation in 2021.

Julie Holtzople is Senior Director, Clinical Transparency and Data Sharing, AstraZeneca.
Christopher Pfitzer is Associate Director, Transparency Operations Lead at UCB Biosciences, Inc.






{kind=link}
{kind=link}
{kind=link}